- Introduction
In this chapter, we consider the therapeutic service system in Tasmania, which has the potential to support victim-survivors of institutional child sexual abuse and children who have engaged in harmful sexual behaviours.
Without the right support and intervention, victim-survivors can be left to cope with their trauma in ways that are harmful to themselves and others—such as using alcohol and other drugs, engaging in violent or criminal behaviour, or self-harming. It can have an impact on their life opportunities, including their ability to engage in education and employment. They can also become vulnerable to more victimisation.1
We heard that the first contacts a victim-survivor has with a therapeutic service can affect their trajectory towards recovery. If they feel supported and validated, they are more likely to engage in therapeutic treatment and to seek justice. However, if they feel dismissed or minimised, they may be less likely to pursue recovery or justice for themselves.2 Therefore, when a victim-survivor reaches out for help, referral pathways need to facilitate timely access to appropriate services. This service system needs to be informed by its users—adult and child victim-survivors.
While our terms of reference require us to inquire into the needs of victim-survivors of child sexual abuse in institutional settings, we consider our recommendations in this chapter will benefit all victim-survivors of child sexual abuse who have similar and complex therapeutic needs.
Victim-survivors may disclose their abuse at any time after it occurs and sometimes do so very late in their lives. Impacts of child sexual abuse can also manifest differently at various stages in a person’s life—for example, when they enter adolescence or when they have their own children. Recognising these diverse needs across the lifespan, this chapter considers the different support needs of child and adult victim-survivors. We also consider victim-survivors who have extra needs or often experience barriers to receiving suitable support, such as those who have disability or are Aboriginal.
We discuss the needs of children who have engaged in harmful sexual behaviours separately in this chapter. These children need an added level of specialised help and intervention to address the harm that the behaviour does to their development, and to reduce the likelihood of them repeating the behaviour. Although children who have displayed harmful sexual behaviours may experience criminal justice issues as a result, and cause harm to victim-survivors, we consider it vital to recognise that these children need help. We also consider that children who have been harmed by the sexual behaviours of another child need equivalent therapeutic supports to victim-survivors of other forms of child sexual abuse.
We do not explore therapeutic interventions available to adult perpetrators of child sexual abuse in this chapter, although we consider it briefly in Chapter 16.
This chapter is divided into four main sections, in addition to the Introduction (Section 1) and Conclusion (Section 6).
In Section 2, we outline the National Royal Commission’s recommendations for an accessible, well-coordinated therapeutic service system designed to meet the needs of victim-survivors.
In Section 3, we describe the services available to victim-survivors of child sexual abuse. We refer to these services as ‘sexual assault services’ in line with current practice, noting that they provide services for victim-survivors of child sexual abuse and of adult-on-adult sexual assault (and do not limit services to abuse that meets a criminal definition of assault).
As outlined in Section 3, we found it difficult to get a handle on the therapeutic service system and how the various components of the service system intersect.3 We note that it may be even more difficult for people who need these forms of support to understand how the service system works and what is available to them.
In Section 4, we consider the extent to which the therapeutic service system meets the needs of victim-survivors of child sexual abuse and offers services that are accessible and appropriate. We identify several areas for improvement including:
- a need for government leadership to develop and fund a well-coordinated therapeutic service system for child sexual abuse
- a need for more sexual assault counselling services to enable adult and child victim-survivors of child sexual abuse to access them easily and in a timely way
- an urgent need for more culturally appropriate Aboriginal healing services and for sexual assault services that accommodate diversity and disability in a natural and welcoming way.
In Section 5, we focus on the therapeutic service system for children who have displayed harmful sexual behaviours. We conclude that children who have displayed harmful sexual behaviours need better access to therapeutic services, and that there needs to be a coordinated response across government agencies, which the Government should lead.
Overall, a well-functioning, trauma-informed, accessible, collaborative and appropriate therapeutic service system for child sexual abuse and harmful sexual behaviours requires the Tasmanian Government to assume a higher level of responsibility for overseeing, funding and monitoring such a system.
- National Royal Commission
The Royal Commission into Institutional Responses to Child Sexual Abuse (‘National Royal Commission’) dedicated volume 9 of its final report to ‘advocacy, support and therapeutic treatment services’ for victim-survivors. Five of the recommendations in that volume are relevant to the Tasmanian Government’s responsibility for the funding and characteristics of the Tasmanian service system for child sexual abuse, namely:
- ensuring there is a system of integrated advocacy, support and counselling for child and adult victim-survivors of child sexual abuse in institutional settings (Recommendation 9.1)
- increasing funding to sexual assault services to improve their capacity to support adult and child victim-survivors of child sexual abuse in institutional settings (Recommendation 9.6)
- funding Aboriginal and Torres Strait Islander-specific healing approaches (Recommendation 9.2)
- funding for support services for victim-survivors with disability (Recommendation 9.3)
- ensuring government human services agencies’ policy frameworks and strategies recognise the needs of victim-survivors and the benefits of trauma-informed approaches in their work (Recommendation 9.8).4
Since 2018, Tasmanian Government has reported annually on its implementation of the National Royal Commission’s recommendations, most recently in the Fifth Annual Progress Report and Action Plan 2023.5 From its progress report in 2020 onwards, the Government began referring to its action plans for family violence as also including ‘sexual violence’ and fulfilling many of the National Royal Commission’s recommendations.6
The Government’s fifth report suggested that its Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027 has fulfilled the above five National Royal Commission recommendations, but it provided little information to address each recommendation.7
Our reading of the Government’s third action plan and its predecessor—Safe Homes Families Communities: Tasmania’s Action Plan for Family and Sexual Violence 2019–2022—revealed that only six of the 38 actions contained in the plans could be considered relevant to the sexual assault service system (depending on how they are implemented); the others relate to family violence.8 The relevant six actions cover improved forensic testing technology (Action 4), increased core funding to sexual assault counselling services with five-year funding contracts (Action 12), establishing a peak family and sexual violence body (Action 14), ‘strengthening’ the Victims of Crime Service (Action 19), continuing the Sexual Assault Support Service’s recently funded Prevention, Assessment, Support and Treatment program for addressing harmful sexual behaviours (Action 28) and establishing two multidisciplinary centres (Action 1).9
We are concerned that the Government decided to incorporate the National Royal Commission’s recommendations about child sexual abuse into the existing activities and frameworks for family and sexual violence. We recognise that child sexual abuse can co-occur with family violence, but this approach misses the intention of the National Royal Commission’s recommendations; namely, that child sexual abuse, and particularly child sexual abuse in institutions requires a specific response. We consider this recognition requires the Government to lead, coordinate and fund therapeutic services specifically for child sexual abuse and harmful sexual behaviours. We discuss these concerns further in Chapter 19.
- The current service system
Tasmania’s therapeutic service system for child sexual abuse took us some time to comprehend despite our own research activities and our notices to produce to the Government (discussed in Section 4). We benefited greatly from the information provided by local sexual assault services: the Sexual Assault Support Service and Laurel House.
Broadly speaking, the Tasmanian therapeutic service system for child sexual abuse appears to have evolved over time, often in silos and in response to local issues. We identified its main components to be:
- the Strong Families Safe Kids Advice and Referral Line (‘Advice and Referral Line’) for concerns or suspicions about the sexual abuse of a child
- local sexual assault counselling services, which provide a crisis response and short-, medium- or longer-term support
- counselling support available through the National Redress Scheme
- local counselling support for victims of crime
- local therapeutic services for children who have displayed harmful sexual behaviours
- national online or phone sexual assault support services
- forensic services to collect evidence that may be used to prosecute a sexual crime (explored in Chapter 16)
- multidisciplinary centres where sexual assault services are co-located with other services that victim-survivors may need, such as police, the Child Safety Service or family violence assistance
- mainstream counselling or mental health services that often need to respond to disclosures of sexual abuse or its impacts while delivering therapeutic support.
In a collaborative and responsive therapeutic service system, as advocated by the National Royal Commission, all aspects of the service system communicate well and refer to each other easily.10 In the rest of this section, we explore each part of Tasmania’s service system in turn before examining areas requiring improvement in Section 4.
- Advice and Referral Line
For people who are concerned about the welfare of a child, the Advice and Referral Line is often their first port of call for advice about what to do and where to go. As well as its statutory role in the child protection system, the Advice and Referral Line refers families and children to services that could assist with problems they are experiencing, including referring a family to sexual assault services to receive support for child sexual abuse or harmful sexual behaviours.11
- Local counselling services
- MY SUPPORT helpline
In the first instance, Tasmanian victim-survivors can phone the State Government funded 24-hour 1800 MY SUPPORT helpline for support in relation to sexual assault or sexual abuse.12 The MY SUPPORT helpline number is directed to counsellors employed at the Sexual Assault Support Service or Laurel House (described in the next section), depending on the caller’s location.13 Phone counsellors provide immediate crisis support for victim-survivors, assist them if they want to make a report to police and/or want a forensic medical assessment, and refer them for in-person counselling and support, including through Laurel House and the Sexual Assault Support Service.14
- Sexual assault counselling services
The two main sexual assault counselling services generally service distinct geographical regions in Tasmania—Laurel House provides services to northern Tasmania and the North West, and the Sexual Assault Support Service provides services in southern Tasmania.15 The Tasmanian Government funds both services to offer counselling and support for a wide range of victim-survivors, including victim-survivors of institutional child sexual abuse and children who have experienced harmful sexual behaviours from another child.16 Following the disbandment of the Department of Communities on 1 October 2022, the Department of Premier and Cabinet began funding sexual assault services.17
There is a third, much smaller service—Enterprising Aardvark—in northern Tasmania, but it is not government funded.
Broadly speaking, the Sexual Assault Support Service and Laurel House appear to offer roughly equivalent services in many respects. Both agencies support victim-survivors of child sexual abuse (including harmful sexual behaviours) of all ages and genders, as well as ‘secondary victims such as parents, siblings, friends and supporters’ by a variety of means: in person, phone, online and outreach.18 We concluded that both agencies employ experienced therapists who have degree-level qualifications in counselling, psychology or social work, and provide their staff with professional development and supervision.19
Laurel House and the Sexual Assault Support Service accept referrals from many different sources.20 When a victim-survivor contacts either service directly, they speak to an intake counsellor who triages the case for allocation to a counsellor.21 While a person is awaiting allocation, both services provide crisis assistance (refer to discussion about waiting lists in Section 4.3.1).22
The Sexual Assault Support Service has the advantage of having greater capacity, perhaps due to the larger population in southern Tasmania. The Sexual Assault Support Service has also secured the entire government funding for providing therapy to children and young people up to the age of 18 who engage in harmful sexual behaviours (the Prevention, Assessment, Support and Treatment program described in Section 5.2.1) and receives Commonwealth funding to provide counselling for victim-survivors seeking redress through the National Redress Scheme (refer to Section 3.2.3 and, for more detail, Chapter 17). It employs 48 staff, most of whom are part-time, and receives about 1,400 referrals a year.23
Laurel House provided counselling to just under 900 clients in the 2020–21 financial year.24 The service did not provide staffing numbers, but its Chief Executive Officer, Kathryn Fordyce, advised us that the case load of a full-time counsellor at Laurel House was the same as for the Sexual Assault Support Service: about 30 clients at any one time.25
We learned of Enterprising Aardvark from a victim-survivor who had heard about the service from police.26 According to its website, Enterprising Aardvark is a free counselling and support service in northern Tasmania for victim-survivors of child sexual abuse and their families.27 Its website says it relies on donations because it receives no government funding, employs two part-time counsellors and has provided about 1,500 hours of counselling each year since it started in 2017.28
We were told that, in 2020, Enterprising Aardvark provided education sessions for Ward 4K staff at Launceston General Hospital about profiles of abusers, grooming tactics and strategies.29 Otherwise, we have little information about this service and we presume it is not well-publicised outside informal networks. It did not make a submission to us.
- Redress support services
We discuss the National Redress Scheme in Chapter 17, but consider here the supports provided to victim-survivors as part of that scheme. Many of those involved in accessing the National Redress Scheme, or supporting those who access the scheme, told us that the process can be traumatising, and that support is vital while victim-survivors retell their experiences of child sexual abuse and go through the distressing process of having those experiences quantified against a scale of seriousness.30
In Tasmania the Commonwealth Government funds the Sexual Assault Support Service, Relationships Australia and the South East Tasmanian Aboriginal Corporation to provide redress support services, which are counselling services for victim-survivors in the National Redress Scheme.31 Laurel House said it does not provide redress support services but aims to do so in the future.32
Under the National Redress Scheme, victim-survivors can also choose counselling services from approved counsellors to be included in their redress offer.33 The Department of Justice coordinates this part of the service system.34
Civil legal action can be protracted and very stressful for victim-survivors (refer to Chapter 17).35 Although there is no specifically funded support service for victim-survivors who take civil action over their abuse, sexual assault counselling services will support victim-survivors who are engaging in civil action.36
- Victims of Crime Service
Provided by the Department of Justice’s Victims Support Services (refer to Chapter 17), the Victims of Crime Service has offices in Burnie, Launceston and Hobart.37 The service ‘provides a counselling, support and referral service to victims of serious interpersonal violence and sexual offences’.38
This free service is generally used by victim-survivors who have reported their abuse to police.39 Basic information about the service is available on the Department of Justice’s website.40
- Online and phone sexual assault support services
Phone and online sexual assault support services for victim-survivors strengthen Tasmania’s service system. Victim-survivors can contact the free national 24-hour 1800RESPECT helpline, which offers immediate support and counselling for sexual assault and family violence via phone and online. The helpline has a referral database for local services and provides self-help information and apps to help victim-survivors access supports in a safe way.41 Organisations, such as the Sydney-based Survivors and Mates Support Network for male victim-survivors and the national organisation Blue Knot Foundation, provide some support, information and referral services to victim-survivors and their supporters.42
- Forensic medical assessments
The Tasmanian Health Service can undertake forensic examinations for victim-survivors after a sexual assault. These examinations can be conducted at the Royal Hobart Hospital, the Launceston General Hospital and the North West Regional Hospital (Burnie).43 The victim-survivor’s chosen service will conduct the medical examination, record injuries and collect biological samples if relevant. A victim-survivor does not need to have made a police report to have a forensic medical examination.44 Counsellors from Laurel House or the Sexual Assault Support Service can support the victim-survivor during the examination.45
Chapter 16 discusses forensic medical examinations including the roles of police, medical and nursing personnel and specialist sexual assault services.
- Multidisciplinary centres
Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan
2022–2027 committed to piloting two multidisciplinary centres as a new action ‘to provide survivor-centred, holistic and integrated responses to family and sexual violence’.46 These centres, named Arch centres, should be up and running in 2023.47 Tasmania Police has led development of these multidisciplinary centres to improve specialisation for police and coordinate responses to sexual violence in general.48 In Chapter 16, we call for Tasmania Police to prioritise police specialisation. Refer to Section 4.2 for more on the new Arch centres.
- Mainstream services
Not everyone who was sexually abused as a child will access only specialist sexual assault services. Many victim-survivors will seek support for the problems arising from experiencing child sexual abuse, such as post-traumatic stress disorder, alcohol and other drug misuse, suicidal ideation, depression, anxiety and relationship issues.49
The key mainstream services that we consider would have contact with victim-survivors for treatment or referral are:
- medical practitioners such as psychiatrists and general practitioners who can provide Mental Health Treatment Plans under Medicare
- private psychologists and mental health practitioners who see clients referred by general practitioners, often subsidised for a set number of sessions by Medicare under a Mental Health Treatment Plan
- public mental health services offered by the Tasmanian Health Service such as Adult Mental Health Services, Child and Adolescent Mental Health Services, the Alcohol and Drug Service and adult inpatient mental health units
- Aboriginal health organisations (discussed more in Section 4.4.7).
We discuss the need for government mainstream services to become more trauma-informed in Chapter 19.
- Improving the therapeutic service system
As a basis for its recommendations (refer to Section 2), the National Royal Commission identified the key characteristics of a responsive service system for adult and child victim-survivors of child sexual abuse and for children who have displayed harmful sexual behaviours:
- The system and its components need to be trauma-informed and knowledgeable about child sexual abuse.
- The system needs to work together to meet the range of potential needs of victim-survivors and the complexity of the service system.
- Enough services should be available for victim-survivors to access and be delivered for as long as necessary for each person.
- Services should be accessible for all victim-survivors regardless of their capacity to pay, geographical location, disability or cultural background.
- Services should be ‘acceptable’ to victim-survivors who have diverse needs; that is, they should be flexible enough to respond to victim-survivors from a variety of cultural and social contexts.
- The high quality of the services should be assured through ongoing evaluation of evidence-informed approaches.
- The service system should include Aboriginal healing approaches.50
The National Royal Commission’s recommendations assigned responsibility to the state and territory governments to ensure the therapeutic service system has these characteristics.51 We consider that the Tasmanian Government needs to do more to meet these requirements.
This section considers the extent to which the current therapeutic service system meets the needs of victim-survivors and provides services that are accessible and appropriate. We also identify several areas for improvement.
- Developing a therapeutic service system for child sexual abuse
The Tasmanian therapeutic service system has evolved organically from the bottom up. Over time, separate non-government services have been established in communities to meet the needs of victim-survivors at that time. Gradually, services have sought and received government funding to expand into areas where they have identified gaps. Consequently, the service system is not particularly cohesive or equitable.
At the strategic level, we consider the Tasmanian Government has not taken responsibility for ensuring the therapeutic service system is adequately planned and funded. Instead, the task of service provision and leadership in the system has fallen to hard-working and dedicated non-government organisations. There has therefore been no coordination or overarching plan for developing the system that would ensure consistency in approach, coordination of services, appropriate coverage or equitable access.
We asked the Government to describe its service system in preventing, identifying, reporting and responding to allegations or incidents of child sexual abuse in institutional contexts, including for:
- advocacy, therapeutic and social supports for victim-survivors
- therapeutic and social supports for children who have displayed harmful sexual behaviours
- targeted supports for
- Aboriginal children
- children with a culturally and linguistically diverse background
- children in youth detention
- children in out of home care
- children with disability
- children who identify as LGBTQIA+
- any other groups that receive targeted supports.52
The Government’s response did not demonstrate to us that there is a well-structured therapeutic service system for adult and child victim-survivors of child sexual abuse and children who experience or display harmful sexual behaviours.53 In the remainder of Section 4 and in Section 5, we outline gaps in the scope of sexual assault services for victim-survivors of child sexual abuse and harmful sexual behaviours, as well as in a consistently coordinated approach to service delivery.
Given the difficulties we experienced trying to understand the therapeutic service system for child sexual abuse, it follows that victim-survivors would also find it difficult to understand the service system and access the services they need when they need them.
The Tasmanian Government should lead, coordinate and fund development of a therapeutic service system that includes responses for adult and child victim-survivors of child sexual abuse and for children who have experienced or displayed harmful sexual behaviours. This therapeutic service system should ensure coordination of services, appropriate service coverage and equitable access to quality services.
The Government should ensure the therapeutic service system is easily understood by victim-survivors and those affected by child sexual abuse, as well as mainstream services that may need to make or receive warm referrals.
The Government also needs to know the therapeutic service system is working and meeting the needs of victim-survivors. The National Royal Commission stated that ‘a high-quality service system is informed by evidence, well-trained and supported, outcome focused, accountable and subject to ongoing evaluation’.54
We only heard about two of the services in Tasmania’s sexual assault service system that are being actively evaluated, mainly because they are both pilot programs—the Prevention, Assessment, Support and Treatment program for harmful sexual behaviours and the Arch centres.
The Sexual Assault Support Service expressed concern about a lack of quality assurance or standards required in government funding contracts.55 We identified a similar concern in the context of non-government out of home care provider funding agreements (refer to Chapter 9). Commissioning arrangements appear to have been problematic in several areas in the former Department of Communities.
The Department of Premier and Cabinet, in its new role of funding sexual assault services, should provide leadership, fill service gaps and ensure funding agreements with non-government sexual assault counselling services have governance requirements, service evaluation and child safe accreditation built in. The child safe accreditation will empower children to contribute to how the services provided for them are shaped.
It is important that in leading development of this therapeutic service system, the Government collaborates with all those affected by the service system including children and adult victim-survivors, specialist counselling services, police, government agencies and the peak body for the sexual assault service system recommended in Recommendation 21.3.
Recommendation 21.1
- The Department of Premier and Cabinet should lead, coordinate and fund a therapeutic service system for child and adult victim-survivors of child sexual abuse and children who have experienced or displayed harmful sexual behaviours.
- The Department should ensure the therapeutic service system:
- addresses service gaps and provides coordination of services, appropriate coverage and equitable access to quality services
- is easily understood and accessible to the public, state servants and other mainstream service providers.
- The Department, in leading this work, should consult with:
- any relevant government departments, including the Department for Education, Children and Young People, the Department of Health and Tasmania Police
- sexual assault and abuse counselling services
- the Premier’s Youth Advisory Council and the adult victim-survivors of child sexual abuse advisory group (Recommendation 19.5)
- the peak body for the sexual assault service system (Recommendation 21.3).
- The Tasmanian Government should ensure funding agreements with non-government specialist services include appropriate governance requirements, sexual abuse service standards, service evaluation and child safe accreditation.
- Creating a collaborative system
The National Royal Commission heard that services victim-survivors need ‘span several sectors and can be difficult to navigate’ and that those services ‘[do] not collaborate with one another, compounding the difficulties victims and survivors faced when navigating the complex policy and service environment’.56
Kylee’s experience
One victim-survivor told us about her experience of having to tell nine people her story in order to report to police and receive therapeutic care.
For someone who never wanted to tell anyone, the amount of people I then had to tell … One example is Victims of Crime, I was encouraged by the Detective to contact them, so I ring up to make an initial appointment, you’re then speaking to a counsellor to do an extension of time application, that then goes to someone to be assessed. Then come in and see someone else to do an application … then I’m contacted by someone who says ‘you need to see a counsellor’ ... They then organise me to see a phone link-up counsellor, she says, ‘you do realise you’re going to have to tell your GP?’ … Then because the counsellor thought I had a diagnosis of moderate post-traumatic stress disorder, I had to then be referred on to a psychologist … Then I had an interview with a Commissioner [for Victims of Crime], and an assistant and they then determined whether I was eligible or not … nine people I had to share my experience with.57
The National Royal Commission recommended establishing:
… dedicated community support services for victims and survivors in each jurisdiction, to provide an integrated model of advocacy and support and counselling to children and adults who experienced childhood sexual abuse in institutional contexts.58
The Blue Knot Foundation’s Organisational Guidelines for Trauma-Informed Service Delivery also supports providing collaborative, integrated care:
People living with the impacts of trauma often present to multiple services over a long period of time. The care they receive is frequently fragmented and not well coordinated between services. There are often inadequate referral and follow-up pathways. These failures in the system can mean that clients experience a ‘merry go round’ of unintegrated care. As a result, people are more likely to be retraumatised and their trauma is more likely to be compounded.59
We heard of local examples of close working relationships between services, such as in North West Tasmania. Community members there proudly reported that police, schools and the Child Safety Service in their area had developed a good working relationship to respond in a trauma-informed way to disclosures of child sexual abuse and, perhaps consequently, they reported an increase in disclosures.60 Laurel House also noted the flow-on benefits for victim-survivors of developing positive working relationships with police and other services.61
The response to child sexual abuse in Tasmania includes some systems for collaboration, such as interagency case discussions and a memorandum of understanding to share information between police and the Child Safety Service. However, we were told that ‘effective collaboration and therefore responses stem beyond this’ and:
… the response to allegations and incidents of child sexual abuse in institutional contexts is complex and requires multi-agency collaboration, inclusive of co-located cross-agency teams, improved information sharing, appropriate specialised training and consultations between key agencies.62
Jillian Maxwell, Chief Executive Officer, Sexual Assault Support Service, noted that:
Victim-survivors of all ages express feeling overwhelmed in respect of the number of agencies who they are meant to ‘follow up with’. The onus is often placed on the individual, who has already experienced significant hardship and distress, to contact the Police, Child Safety Services and other State Government agencies … [multidisciplinary centres] would be particularly beneficial given the way we work in Tasmania; a place which is built on relationships, trust and safety. Having a client, whether an adult or a child, attending at one place where they are supported by their counsellor in accessing the other services that are either co-located or coming onsite would also be much more trauma-informed than current ‘siloed’ approaches.63
For the past few years, the Sexual Assault Support Service and Laurel House have lobbied for the setting up multidisciplinary centres in Tasmania to better coordinate services and provide ‘collaborative and integrated responses to victim-survivors in one location’.64
- The Tasmanian model of multidisciplinary centres
As discussed above, the Government committed to piloting two multidisciplinary centres as part of its Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027.65 On 2 December 2022 the Government announced that two Arch centres, one in Hobart and one in Launceston, would be ‘available in 2023’.66 In conjunction with sexual assault services, Tasmania Police has led development of the centres as a means of improving specialisation for police and for coordinating responses to sexual violence more generally.67 The Government has said that these multidisciplinary centres will enable victim-survivors to ‘receive immediate and integrated support in a safe place’.68 The intention is to facilitate a positive first contact with counselling and statutory services for victim-survivors.
We discuss the evidence for the effectiveness of multidisciplinary centres and the need for police specialisation in Chapter 16. This section focuses on the proposed Tasmanian model of multidisciplinary centres and how they might meet the therapeutic needs of victim-survivors.
Arch centres
The Tasmanian Government has indicated that the pilot Arch centres aim to be a ‘one-stop shop’ for victim-survivors of sexual abuse to access all the services they need in one location.69 On the basis of available information at the time of writing, it appears that services at the centres may include:
- sexual assault counselling services
- specialist sex crimes police investigators
- child safety support workers
- family violence counselling support services
- witness intermediaries (as requested)
- facilities for tailored service provision (as required)
- State Service employees in investigative support roles.70
Arch centres are being co-designed with victim-survivor advocates and existing services in the family and sexual violence sector to ensure ‘service delivery meets the needs of victim-survivors’.71 As part of the process of ensuring these are child safe organisations, we encourage the Government to work with children to inform their design. We also caution the Government to ensure the design process goes beyond co-locating services to the purposeful systems, processes and practices that will support multidisciplinary collaboration, preventing victim-survivors from having to retell their story to each service in the Arch centre with which they engage.
Key elements of the proposed model are set out in Figure 21.1.
Figure 21.1: Key elements of the Arch centre model72
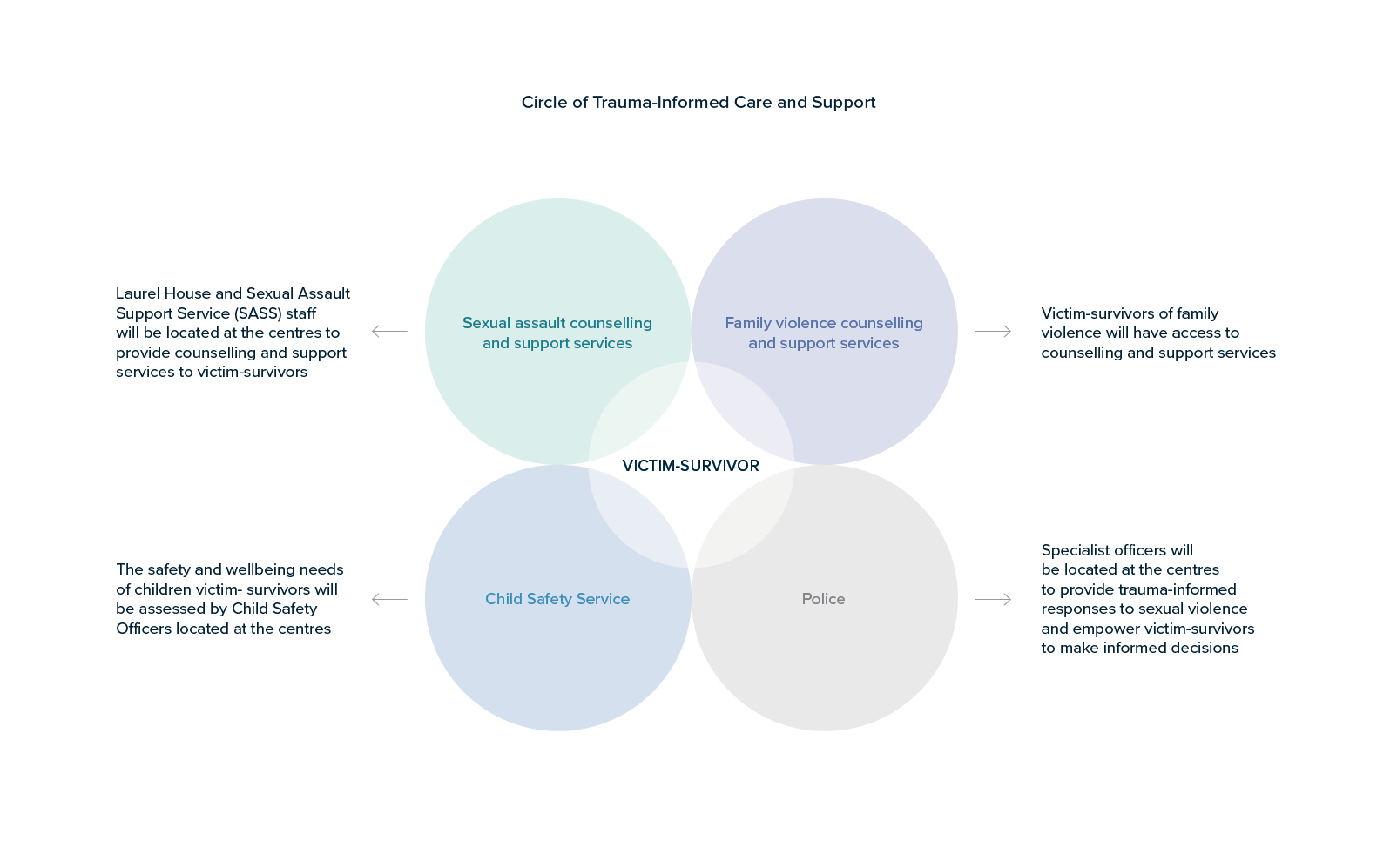
The $15.1 million allocated to Arch centres for the two-year pilot includes funds for new full-time-equivalent positions:
- 15 specialist sex crimes investigators (10 in the south and five in the north)
- nine State Service employees in analytics and specialist roles (across the model)
- three Child Safety Officers (two in the south and one in the north)
- two family violence counselling support workers (one each in the south and north).73
It is unclear how many staff from sexual assault counselling services will be at the centres, but we note that, in addition to the above, $21 million has been allocated to the sexual violence sector and $51 million to the family violence sector ‘to support the implementation of the Third Sexual and Family Violence action plan’.74
Key considerations
Although there are many potential benefits to the multidisciplinary centre model, its success depends on several factors. Professor Leah Bromfield, one of the Commissioners for our Inquiry, co-authored an article with James Herbert based on a national analysis of the multidisciplinary centre model. In the article, Commissioner Bromfield commented: ‘There is often a difference between the stated models and how models operate in practice’.75 The Victorian Law Reform Commission also recently identified some common challenges with multidisciplinary centres including:
- power imbalances between agencies
- tensions in agencies’ purposes and goals
- information sharing and privacy concerns
- being responsible and accessible to victim-survivors with diverse and complex needs
- not having enough resources.76
There is an absence of evidence directly comparing models of cross-agency responses to determine what contributes to positive outcomes, which makes it difficult to work out the essential components for an effective response.77 However, a recent scoping review identified 11 factors that may support quality cross-agency responses and outcomes in cases of child sexual abuse.78 These are listed in Table 21.1. Arch centres will need to consider such factors in their design, implementation and evaluation.
Table 21.1: Factors that may support quality cross-agency responses and outcomes79
|
Process factors (factors reflecting the delivery of a cross-agency model) |
Protocols |
Clear and comprehensive cross-agency protocols that have been developed and agreed to by agencies taking part in the response |
|
Case review meetings |
Provide an opportunity for decision making across agencies and disciplines and for participants to understand each agency’s role |
|
|
Cross-agency training |
Similar training is provided to different professional disciplines |
|
|
Co-location |
Staff are easily accessible and can develop rapport with those from other agencies and disciplines |
|
|
Individual factors (factors enabling workers to effectively collaborate with one another) |
Professional skills and knowledge |
Staff have the skills and knowledge to undertake their own work and to collaborate with others |
|
Mandates, vision, roles and priorities |
Staff can reconcile their own professional responsibilities with their role in a cross-agency team |
|
|
Enabling factors (factors supporting processes and collaboration) |
Feedback and evaluation |
Data is received from victim-survivors and staff to enhance responses |
|
Leadership and governance |
Emphasises the importance of cross-agency leadership, teamwork and dispute resolution |
|
|
Resources |
A lack of resources to support cross-agency collaboration is a barrier to models |
|
|
Improved cross-agency collaboration factors (factors reflecting good practice) |
Trust and respect |
Relationships between staff centre on mutual trust and respect |
|
Communication and information sharing |
There is frequent communication and exchange of quality information across agencies |
Genuine collaboration
Although Arch centre materials indicate that the centres will be physically designed to facilitate collaboration and coordination, Jenny Wing, Chair, Victorian Harmful Sexual Behaviour Network, told us that co-location or proximity does not guarantee collaboration: 80
… [collaboration] is a constant relationship that needs to be maintained. Being co-located in multidisciplinary centres provides greater opportunities to maintain these relationships … there still needs to be a combined effort to meet and engage regularly for the relationship to work effectively.81
The New South Wales experience was similar. Peter Yeomans, Detective Chief Inspector, New South Wales Police Force, who leads the Child Abuse and Sex Crimes Squad, said that ‘effective and regular communication between agencies is critical’, whether the service is co-located or not.82 Tasmania Police acknowledged that the effectiveness of multidisciplinary centres was ‘dependent upon relationships at a practice level, these relationships need to be established prior to systems and structures being imposed’.83 Former Commissioner Darren Hine AO APM from Tasmania Police commented that:
… it’s not having those people in one area; it’s having the right people in that area. And that’s one of the things we’ve learned from other states: some centres work better than others, and it comes down to … leadership, and it comes down to the people actually involved and we need to learn from that.84
Given the importance of coordination and collaboration, it is essential for Arch centres to facilitate these relationships in an ongoing way through strong leadership and deliberate and purposeful collaboration mechanisms that put victim-survivor needs at the centre.
Police presence
A police presence in multidisciplinary centres is pivotal to their success. Tasmania’s sexual assault counselling services recommended that the police presence must be unobtrusive and inconspicuous.85 Indications are that the Arch centres will reflect this principle. Commissioner Hine said: ‘it’s not connected to a police station, will not look like a police station’.86
Laurel House noted that those victim-survivors who do not want to engage with police or direct government services should still be able to access the other services—choice is critical.87 Indeed, choice is a principle of trauma-informed care that must be central to the multidisciplinary centre model.88 Arch centre materials indicate that they have:
… carefully considered the choices clients might make at the centres and what this will mean for their movement within them. If you choose to see one particular service provider only, the design will help to ensure that you do not bump into any others. For example, we respect that some clients may not want to, or may not be ready to, see a police officer. With this in mind, police officers who work in the centres will not be in uniform and will use an alternative door.89
Family violence
Following their examination of the Victorian multidisciplinary centre model, Tasmania Police reported their impression that Victoria Police ‘considered the integration of sex crimes and family violence appropriate given there is extensive research regarding the correlation between the two’.90
Victoria Police told us:
… given the high prevalence of sexual offending in family violence, Victoria Police is continually looking for opportunities to align its responses to these crime themes when they co-occur. Family violence and sexual offence units are specialist units but will operate collaboratively in some instances, such as, when the sexual violence is intrafamilial. Some multidisciplinary centres … include both specialist teams but the key function of [multidisciplinary centres] is to provide specialist sexual offence responses.91
We also heard from several people who have worked in the sexual assault field across different jurisdictions that family violence can become ‘the dominant force’ and that it is better to not ‘dilute the expertise of dealing with child sexual assault matters’.92
Commissioner Hine told us that Arch centres will not incorporate Tasmania Police Family Violence Units, nor will the Safe at Home model change.93 We understand the Safe at Home model to be a cross-government partnership to coordinate responses to family violence.94 Tasmania Police told us that the intention is for extra resources to be allocated to the Safe Families Coordination Unit to expand its role to include sexual violence, enabling it to ‘coordinate information to deliver the Government’s vision of a collaborative, multi-agency response to sexual violence’.95 Commissioner Hine stated that:
This approach provides confidence that high-volume family violence matters will not impact the priority afforded to sexual assault and it is acknowledged that this will need to be subject to evaluation as part of the pilot program.96
Arch centre materials indicate that ‘offences or information relating to family violence’ that require a response will be sent to local police as is the current system, which we take to mean matters will continue to be referred to local Family Violence Units. The material also indicated that if the matter includes ‘sexual violence’, it will be sent to an Arch centre.97
We welcome the commitment to ensure family violence matters do not overwhelm a specialisation in child sexual abuse.
Resourcing
Adequate resourcing of Arch centres will be essential. Ms Maxwell, from the Sexual Assault Support Service, noted that the funding allocated may not be enough to create ideal multidisciplinary centres.98
It is not yet known how the extra funding to the sexual and family violence sectors will be allocated, and whether it will be enough to resource the Arch centres and existing services. However, Arch centre materials indicate that choice will be paramount in terms of services accessed within and outside of the centres. Materials suggest that Arch centres will be an extra rather than a replacement resource and that ‘established counselling and support services already available in the community will not change when the centres commence’.99
Evaluation
The National Royal Commission noted that while multidisciplinary models can achieve goals such as reducing retraumatisation, assisting victim-survivors to navigate the system and promoting effective collaboration between services, ‘co-location and other models of collaboration are only tools to achieve a better service offering, not goals in themselves’.100 Given the complexities of providing effective therapeutic and statutory services to victim-survivors of child sexual abuse, evaluation of Arch centres must be independent, robust and ongoing.
Commissioner Hine told us that, as a pilot program, ‘evaluation will be critical and commence from the program launch to ensure experience informs the future’.101 This is supported by Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027, which indicates that ‘learnings from the pilot will inform future considerations of the model’.102 The evaluation should follow sound principles to provide an accurate picture of the impact of Arch centres.
We heard from stakeholders that multidisciplinary centres ‘will not provide the solutions to all the issues and challenges that affect victim-survivors of child sexual assault in Tasmanian Government settings’.103 Similarly, the Victorian Law Reform Commission recommended expanding multidisciplinary centres in Victoria, but acknowledged that they are only one feature of a much larger system.104 We discuss other aspects of the service system, including sexual assault counselling services, in Section 4.3.
Recommendation 21.2
- The Tasmanian Government should conduct an independent process and outcomes evaluation for the pilot multidisciplinary Arch centres and any future centres after three years of operation to inform the Government of any systems improvements that could be made to the centres and whether they have resulted in improvements in client outcomes. The evaluation should incorporate:
- an evaluation and data outcomes framework established during the first year that includes required baseline and outcomes data for clients receiving services through the Arch centres, and considers how Arch centre outcomes can be compared with the outcomes of cases that have not received an Arch centre response
- the collection of data in line with the data outcomes framework in the first year
- the storing and retention of data in a format that can be provided to the independent evaluators.
- The evaluation and data outcomes framework should include outcome measures for adult and child victim-survivors of child sexual abuse and children who have experienced or displayed harmful sexual behaviours.
- The Tasmanian Government should ensure multidisciplinary centres are not the sole response to the therapeutic needs of adult and child victim-survivors of child sexual abuse.
- Peak body
Despite the small size of its service system, Tasmania’s specialist sexual assault service providers can be relatively isolated from one another, and from interstate services, due to the north–south Tasmanian divide and the lack of a coordinated service system. Other states have peak bodies representing sexual assault services to coordinate services and advocate for system improvements, but Tasmania does not have such an organisation.105
The closest approximation in Tasmania is Providers of Sexual Assault Care. The organisation’s website lists its main members as Tasmania Police, Sexual Assault Forensic Examiners at Launceston General Hospital, the specialist sexual assault support services of Laurel House and the Sexual Assault Support Service, and Forensic Science Service Tasmania.106 Although its membership reflects a strong forensic focus, Providers of Sexual Assault Care has a broader stated purpose: to bring together the services that respond in the event of a sexual assault to support those involved in the care of victim-survivors of sexual assault, share multidisciplinary knowledge, facilitate ‘expert total care’ to victim-survivors and raise awareness of the problem of sexual assault.107 The Providers of Sexual Assault Care administrator advised us that the organisation is funded through membership fees. The Tasmanian Government did not refer to it in its ‘Tasmanian Government’s current service system’ response to our notice to produce, discussed in Section 3.108
The Government has recognised the need for a peak body in Action 14 of Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027, which committed the Government to funding the Tasmanian Council of Social Services to establish a peak family and sexual violence body.109 The peak body would:
… streamline engagement between Government and the community sector, and support the sector in policy development, enabling it to focus on service delivery to the Tasmanian community.110
This is a promising move, but we remain concerned about the Government combining family violence with child sexual abuse. Such a peak body risks being dominated by a focus on family violence, given the sheer size of this important social problem.
The Tasmanian Government should establish a more active, supported peak body to improve the sexual assault service system in a more consistent and coordinated way and, in this, consider the existing Providers of Sexual Assault Care. The coordination function of a peak body would be important as the Government expands sexual assault services available to victim-survivors, as described in Recommendation 21.4. A peak body could also develop or adopt existing standards of practice to ensure consistent quality in sexual assault services, as the Victorian Harmful Sexual Behaviour Network has done in Victoria.111
Recommendation 21.3
- The Tasmanian Government should establish a peak body for the sexual assault service system, including therapeutic interventions for children who have engaged in harmful sexual behaviours, to:
- ensure the needs of adult and child victim-survivors of child sexual abuse and children who have experienced or displayed harmful sexual behaviours are met by the sexual assault service system
- represent sexual assault service providers in a coordinated way
- share evidence and experience
- develop or identify practice standards for sexual assault services and interventions for child sexual abuse and harmful sexual behaviours
- coordinate service delivery for victim-survivors
- advocate for improvements in the sexual assault service system.
- This peak body for the sexual assault service system should be distinct from, but work in cooperation with, a family violence peak body.
- Building on sexual assault services
Our resounding impression is that there are not enough local sexual assault services available or accessible to Tasmanian victim-survivors of child sexual abuse or children who have displayed harmful sexual behaviours. This shortage applies to timely, local forensic medical examinations, sexual assault counselling services, therapeutic interventions for children who have engaged in harmful sexual behaviours and counselling services available through the Victims of Crime Service.
Also, victim-survivors in Ashley Youth Detention Centre and more remote parts of the State experience particular difficulty in accessing suitable supports. The Government needs to address this shortfall in specific ways, which we describe in this section.
In Section 4.4, we discuss the problems of accessing services that meet the needs of some victim-survivors including victim-survivors with disability, or those wanting to access an Aboriginal service.
In Section 5, we consider and make recommendations about services for children who have engaged in harmful sexual behaviours.
- Sexual assault services
Sexual assault counselling services
Ms Maxwell told us that victim-survivors of child sexual abuse in institutional settings can be especially sensitive to a service’s response because they have often experienced poor institutional responses.112 Therefore, she said, quick access to services is important for those people because they can perceive delays as not being heard or supported.113
During sessions with a Commissioner and in consultations, we heard concerns about waiting lists for sexual assault counselling, which people attributed to lack of funding.114 Victim-survivors told us how difficult it was to wait for sexual assault counselling once they had disclosed their abuse.115
In May 2022, the Sexual Assault Support Service told us that it had about 90 people on its waiting list and it expected some of those would need to wait six-to-eight weeks before they could start work with a counsellor.116 At the same time, Laurel House said it had about 40 people on its waiting list and some were waiting up to 33 working days (more than six weeks) to see a counsellor.117 This is too long to wait for services.
Laurel House and the Sexual Assault Support Service said they develop a plan with each person on the waiting list to ensure they have access to support while they wait to see a counsellor.118 A child sexual abuse counsellor told us that there should not be a waiting time for a child victim-survivor and their family to access specialist support.119 Both services said, where possible, they prioritise children on their waiting lists ahead of adults.120
It appears that a significant increase in referrals without a corresponding increase in funding has contributed to larger waiting lists.121 Both services also told us that they can struggle at times to attract and retain qualified and experienced counselling staff, which has further increased waiting times.122 Kathryn Fordyce, the Laurel House Chief Executive Officer, told us that one factor contributing to difficulties with staff attraction and retention is the short-term nature of government funding; staff can be anxious about continuing in a role if funding is not secure.123
In November 2022, the Tasmanian Government announced a 37 per cent increase in core funding to family and sexual violence services and has introduced five-year contracts to assist with funding certainty.124 However, the Government did not specify how the funding will be allocated to services.125 Because the funding increase covers family violence services as well as sexual assault services, it is not clear what proportion will be allocated to specialist services for victim-survivors of child sexual abuse.
Victims of Crime Service
For a variety of reasons, some victim-survivors may prefer not to engage with the sexual assault service in their area. Having access to other free or low-cost counselling services offers victim-survivors some choice, which is an important characteristic of a trauma-informed sexual assault service system. The Victims of Crime Service provides an alternative counselling service option for those victim-survivors who cannot or prefer not to engage with the Sexual Assault Support Service or Laurel House.
Victim-survivors told us that they thought the Victims of Crime Service was underfunded.126 However, Catherine Edwards, Manager, Victims Support Services, told us that the average waiting time for a victim-survivor to see a Victims of Crime Service counsellor was one-to-two weeks, which seems reasonable.127 The service has one full-time counsellor in southern Tasmania, one almost-full-time counsellor in northern Tasmania and a 0.4 full-time-equivalent counsellor in the North West.128 Ms Edwards also said there was ‘an urgent pressing need’ to increase the Victims of Crime Service counsellor position in the North West to full-time and, ideally, she would like to see two counsellors in each region.129 She said the scope of the Victims of Crime Service is confined by its budget, and more resourcing would allow the service to provide more for victim-survivors.130 We expect that more promotion of the service would increase demand, so it would seem wise to expand the service to at least Ms Edwards’ ideal staff complement.
We welcome the Tasmanian Government’s commitment to ‘Strengthen the Victims of Crime Service’ in Action 19 of Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027; however, we note that the plan has no information about what this might involve.131 We recommend that it increases the number of counsellors available to support victims of crime and promotes the service to victim-survivors (refer to Recommendation 21.5). While some victim-survivors of child sexual abuse in institutional settings will choose not to seek support from a government service, others will welcome an alternative among the limited range of options.
- Geographical isolation
As a very small jurisdiction with a widely distributed population, Tasmania has always posed a significant challenge to the fair and equitable distribution of services. This challenge is amplified when trying to ensure all Tasmanians have access to sexual assault services. Such services might only be required intermittently and are more expensive to provide and access than in larger jurisdictions, which can benefit from the economies of scale associated with larger population centres. While this problem is not unique to Tasmania—victim-survivors in rural and regional areas across Australia are disadvantaged when it comes to accessing sexual assault services—the Government should address the need for these services across the State.132 The situation appears to be particularly challenging in Tasmania’s West Coast and North West. For example, in Queenstown we heard that a lack of transport options and difficulty attracting skilled staff make it difficult for victim-survivors to access sexual assault services.133 In a general discussion about the challenges of reduced services overall, Aboriginal community members in the North West spoke of difficulties accessing sexual assault counselling for children.134 In January 2023, the King Island Courier reported an increase in the number of people disclosing sexual abuse on the island and islanders wanted ‘to develop structures and systems’ to enable victim-survivors to access reporting and forensic services.135 The article reported that the local council had attempted to fill the service gap but had struggled to find the resources.136
The two main Tasmanian sexual assault counselling services offer outreach services to parts of regional Tasmania. Laurel House has offices in Burnie, Devonport and Launceston and provides outreach services to some regional areas in northern Tasmania and the North West, such as George Town, Ulverstone, Beaconsfield and Smithton. However, they have found it harder to offer regular outreach to more remote locations such as Circular Head, the East Coast and the Bass Strait islands.137
In the south, the Sexual Assault Support Service has offices in Hobart and Huonville and will travel to locations such as the Southern Midlands to provide counselling when a client cannot travel to an office.138 The Sexual Assault Support Service will also subsidise clients’ travel to an office if cost is a barrier.139
Both services can provide online or phone counselling for people in remote areas.140 However, some clients do not have access to a computer or a private space at home where they can take part in a session, so they may prefer to travel or meet a counsellor somewhere locally.141 Some community members said phone support services were not personal enough.142
Located in Launceston and Hobart, the two pilot Arch centres will leave large areas of the State without ready access to that service. Commissioner Hine noted that many areas of Tasmania will be too small to have an Arch centre but that consideration is being given to how those areas will have ‘the same service or a similar service’.143 This will need to be carefully considered to ensure victim-survivors can access effective support, regardless of their location.
One of the challenges of holding outreach clinics or visiting clients in remote locations is the cost to the service of the counsellor’s travel time, which makes it more expensive per client to conduct a remote outreach clinic than to provide in-house counselling services.144
However, having access to sexual assault counselling from agencies outside the local community through outreach clinics can be helpful for victim-survivors in small communities. Ms Fordyce said that when specialist services are delivered and located in the local community, service users have encountered difficulties with knowing a service provider in a personal capacity, conflicts of interest and a lack of privacy.145 Ms Maxwell agreed that being external to a local community is a strength in some cases:
It means people can address issues arising in the community without having to approach a member of the community, who might be linked to the issue or person involved in some way.146
Azra’s experience
Azra’s experience illustrates some of the difficulties victim-survivors face in seeking help in a small community:
‘Abe’ (a pseudonym) recommended a psychologist who was a friend of his to help me.147 Initially I spoke to this therapist about Abe using a nickname for him. When I eventually mentioned that I was talking about Abe, the therapy broke down.
I felt so used and discarded by Abe. I was let down by him and by the therapist he recommended. I had invested over 12 months into the therapy and thanks to Abe it was a waste of my time. I had to start again with a new therapist. Abe made something that was already traumatic worse.148
When increasing funding to improve access to sexual assault services, the Tasmanian Government should pay particular attention to improving access for those in regional and remote areas, particularly the far North West, Bass Strait islands and the West Coast. Based on the principle of retaining choice for victim-survivors, this should ideally involve a combination of outreach by sexual assault services to provide in-person counselling, phone and online services; improving transport for victim-survivors to service locations; and increasing the capacity of local mainstream health services to provide trauma-informed care.149
- Ashley Youth Detention Centre
As discussed in Chapter 10, children at Ashley Youth Detention Centre often enter the Centre having experienced child sexual abuse. They may then experience sexual abuse or experience or display harmful sexual behaviours while at the Centre. As a result, they have a high need for sexual assault counselling services.
The Department of Health provides mental health support to children while they are in Ashley Youth Detention Centre.150 However, the Sexual Assault Support Service thought it was advantageous for an external specialist agency to offer outreach to the Centre because children can receive continuity of care in the community when they are discharged.151 Tasmania Legal Aid agreed that this model would be better for their clients in Ashley Youth Detention Centre.152 It also affords children some privacy and oversight of care from a provider external to the Centre, which has been lacking.
Laurel House said it has sometimes given therapeutic support to children at Ashley Youth Detention Centre. The Sexual Assault Support Service said it had not previously had referrals and that it found it difficult to deliver interventions for harmful sexual behaviours in that setting.153 Some people provided examples of a lack of action by staff at Ashley Youth Detention Centre to facilitate therapeutic supports for children in the Centre.154
In contrast with Ashley Youth Detention Centre, the Sexual Assault Support Service said that it had been visiting Risdon Prison since the National Royal Commission to provide sexual assault counselling to inmates. It said that demand has grown to the point where it now has almost three full-time counsellors for that site.155 It said that over time, the prison has become more open to referring inmates who can now also self-refer to the Sexual Assault Support Service.156
Former Secretary of the Department of Communities, Michael Pervan, stated that since our hearings in May 2022, ‘the Sexual Assault Support Service is now available to support young people who were victims or witnesses’ of harmful sexual behaviours in Ashley Youth Detention Centre, and that a private psychology practice provides three hours per week of psychology services to residents via a digital platform.157 He told us that a child who has experienced harmful sexual behaviours at Ashley Youth Detention Centre would receive therapeutic support from the private psychology practice, the Centre’s nurse and the visiting doctor.158
Although it took our Inquiry to trigger them, these changes sound like progress for children in Ashley Youth Detention Centre who need therapeutic support for sexual assault. However, we consider more should be done. The Tasmanian Government should ensure sexual assault services receive enough funding to offer outreach services to children in detention or remand now and into the future. We discuss the need for Ashley Youth Detention Centre to embrace therapeutic supports for young people in Chapter 12.
- Peer support
Some Tasmanians access support from peer support organisations such as the Survivors and Mates Support Network and the Care Leavers Australasia Network. The latter supports care leavers and their families via services that include advocacy, counselling and casework; in Tasmania, it also operates peer support groups in Hobart and Launceston.159 We heard from the Care Leavers Australasia Network that the Tasmanian Government does not fund its services and that it would like to better support victim-survivors.160 We also heard from a victim-survivor who received support from local peer support organisation Beyond Abuse and found this helpful.161 We note that the Survivors and Mates Support Network is the only sexual abuse support specifically for male victim-survivors of child sexual abuse in Tasmania. Men can face different challenges when disclosing child sexual abuse and engaging with support services than women (discussed in Section 4.4) and would benefit from having the choice to access male-specific services.
The National Royal Commission ‘highlighted the importance of peer support in helping victims and survivors to overcome feelings of guilt and betrayal, and reduce isolation through sharing their experiences with one another’, particularly for victim-survivors of child sexual abuse in residential institutions.162 It recommended that dedicated community support services for victim-survivors of child sexual abuse be required and enabled to ‘support and supervise peer-led support models’ as part of their services.163 It also suggested that services ‘should provide practical assistance to peer-led support groups, including by providing professional supervision where required’.164
Given the potential of peer support groups to assist recovery and facilitate advocacy for victim-survivors, this area warrants more investigation and investment in Tasmania. Funding for specialist sexual assault services should include assistance for peer support groups.
Recommendation 21.4
- The Tasmanian Government should increase the funding for free or low-cost sexual assault counselling services to:
- reduce waiting times to no longer than four weeks for victim-survivors, regardless of where they live in Tasmania
- enable fortnightly access to sexual assault counselling in Ashley Youth Detention Centre
- assist peer support groups.
- The Department of Premier and Cabinet should adopt strategies to increase the number of professionals with skills to provide therapeutic responses to abuse-related trauma to address the challenge in attracting and retaining sufficient suitably qualified staff to fill vacancies and meet the need for therapeutic responses to child sexual abuse.
Recommendation 21.5
The Tasmanian Government should increase the capacity of the Victims of Crime Service by:
- increasing the number of counsellors available in each of the Victims of Crime Service offices to at least three in southern Tasmania, two in northern Tasmania and two in the North West
- promoting the availability of the Victims of Crime Service counselling service to victim-survivors of sexual assault.
- Meeting the needs of specific groups
of victim-survivors
We know from the National Royal Commission that children who are Aboriginal, have disabilities, are from culturally and linguistically diverse backgrounds or identify as LGBTQIA+ and who have experienced trauma or neglect are at higher risk of sexual abuse and are more likely to receive an inadequate response to sexual abuse than other children.165
The National Royal Commission described an ‘acceptable’ service system as one that:
... considers the diversity of individuals who have been affected by institutional child sexual abuse and is responsive to their lived, social and cultural contexts. Services should be culturally appropriate and aware of needs related to disability, gender and sexuality, particularly in regional areas where choice of services is limited.166
In this section, we consider the acceptability of the Tasmanian service system for sexual assault, and areas in which it might be improved for victim-survivors and children who have displayed harmful sexual behaviours in the following cohorts:
- children—they require a more family-based and developmentally appropriate approach than adult victim-survivors
- people with disability or a mental health issue
- people who identify as LGBTQIA+
- male victim-survivors
- people from culturally and linguistically diverse communities
- Aboriginal people.
We also consider how the Arch centres can be designed to ensure they are acceptable to a diverse range of victim-survivors.
There is significant scope for the service sector in Tasmania to improve care provided to victim-survivors who have specific needs. For mainstream services, this includes equipping and training the workforce and collaborating with sexual assault services. Also, the National Royal Commission noted that there is ‘very little research’ on effective treatment for some of these groups and that more is needed to inform practice.167
- Children as a subspeciality
The Sexual Assault Support Service told us that about one-third of the referrals they receive are for child victim-survivors.168 As indicated above, the Sexual Assault Support Service and Laurel House prioritise children on their waiting lists.169
The National Royal Commission established that, to be effective, sexual assault services for child victim-survivors need to slightly differ from those for adult victim-survivors, namely:
- they should be flexible and appropriate for the child’s developmental stage
- practitioners working with children ‘need to have specialist expertise and be appropriately qualified’
- therapy needs to involve non-offending carers and family
- it can be helpful to involve the child’s school
- traumatised children can benefit from programs in non-clinical settings that help build their sense of confidence more generally.170
We heard evidence to suggest that Laurel House and the Sexual Assault Support Service attempt to involve schools and families in a child victim-survivor’s treatment and, in the case of harmful sexual behaviours, Mission Australia assists with case management.171
Such a systemic approach with a child victim-survivor is more time-intensive than the direct therapy usually provided to an adult victim-survivor. Therefore, services will need more funding to provide a suitable child-appropriate service than for the same number of adult clients.
- Victim-survivors with disability
The limited evidence available about the prevalence of the child sexual abuse of children with disability suggests that these children are three times more likely to experience child sexual abuse than other children.172 The rates are even higher for female children and children with intellectual and behaviour-related disabilities.173
A range of factors is thought to account for this increased risk:
- children with disability have more exposure to health, medical and other disability-related services, making them more susceptible to mistreatment from service staff
- children with disability are often socially isolated due to stigma and discrimination
- the increased risk arising from their disability is compounded by other risk factors common to many children with disability, such as gender, age, socioeconomic disadvantage and Aboriginality
- their disability may make it harder for them to communicate and disclose child sexual abuse
- families often depend on services and so are reluctant to complain
- the increased regular personal touch associated with physical therapies and personal care can cause a child to develop a ‘broken touch radar’ so they do not recognise inappropriate touch or realise that their bodies belong to them and they are entitled to privacy
- adults often expect children with disability to be more compliant than other children
- adults can misinterpret a child’s attempts to communicate distress or attempts to disclose as disobedience or part of their disability.174
In response to the specific needs of victim-survivors with disability, the National Royal Commission recommended, as Recommendation 9.3, that:
The Australian Government and state and territory governments should fund support services for people with disability who have experienced sexual abuse in childhood as an ongoing, integral part of advocacy and support and therapeutic treatment service system responses for victims and survivors of child sexual abuse.175
The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability may make more recommendations on providing sexual assault services to people with disability. In the interim, the National Royal Commission’s Recommendation 9.3 needs to be fully implemented.
The Tasmanian Government reported its progress towards implementing this recommendation in its Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027.176 This plan commits to a ‘new Disability Action Plan’ for the State and, more relevantly, to:
Deliver funding for community-based projects to support inclusion, access and equity to support diverse Tasmanians who experience barriers for accessing support for family and sexual violence … This includes … Tasmanians with a disability …177
While we welcome recognition of the needs of people with disability, we found it difficult to understand the nature and extent of the Government’s commitment. Moreover, it was the only action in the plan that related to victim-survivors of sexual assault who have disability.
Children with disability are also more likely to engage in or be subjected to harmful sexual behaviours.178 We heard in the out of home care stakeholder consultation that it is difficult to find therapists in Tasmania who can deliver specialised interventions to these children.179 This issue is not unique to Tasmania—there is generally a lack of trauma-informed resources and specially trained therapists to deliver such interventions.180
The National Royal Commission observed that the disability service system can be siloed from other service systems.181 Consequently, disability services remain largely non-trauma informed.182 Conversely, trauma and mental health services struggle to know how to respond to their clients who have disability.183
There are some examples of attempts to cross this divide. For example, Laurel House has a Disability Workforce Support Project to raise awareness of, and the responses of carers and professionals to, the sexual assault and abuse of people with disability.184 It is designed to improve the response of those directly supporting victim-survivors who live with disability. The toolkit and resources webpage provides extensive information about sexual violence and people with disability, including communication guides, trauma-informed approaches, how to respond to a disclosure, referral pathways and links to advocacy services and specialist disability supports for victim-survivors.185
In view of the silos that exist, we suspect that a multipronged solution will be required to improve the quality of therapeutic services for children with disability who have engaged in harmful sexual behaviours and sexual assault services for victim-survivors of child sexual abuse who have disability. This would likely include measures to increase the inclusiveness of sexual assault services, as well as to make disability services more trauma-informed and knowledgeable about child sexual abuse.
The Tasmanian Government should ensure victim-survivors with disability can access appropriate supports, including children with disability who need help with harmful sexual behaviours. On 13 September 2022, the Tasmanian Minister for Disability Services announced the appointment of ‘the State’s first Interim Disability Commissioner’.186 We consider the new Interim Disability Commissioner should be closely consulted in achieving this outcome.
- Victim-survivors who identify as LGBTQIA+
The National Royal Commission heard that there are:
… particular barriers to disclosing child sexual abuse and seeking support faced by victims and survivors who identify as lesbian, gay, bisexual or transgender … marginalisation and a lack of understanding in the service system may act as a barrier to effective support.187
It also found that victim-survivors who identify as lesbian, gay, bisexual or transgender—due to experiencing significant levels of sexual violence, abuse, discrimination, shame, transphobia, homophobia, keeping a low profile and invisibility—may be less likely to access support services.188
We heard during hearings that children and young people who identify as LGBTQIA+ are more vulnerable to being groomed and sexually abused, as well as being less likely to report abuse, partly due to not feeling safe and accepted.189 Also, in a school setting—where these children are at greater risk of experiencing harmful sexual behaviours—disclosures are often not responded to appropriately, further marginalising victim-survivors and dismissing their experiences.190
One transgender victim-survivor told us that the abuse she experienced, as well as the inadequate response she received when she disclosed to the institution and to police, were part of a broader context of her experiences of homophobic and transphobic bullying.191 We also heard from a non-binary victim-survivor who experienced violence and sexual abuse by several abusers; this was partly linked to the vulnerabilities associated with not conforming to gender norms.192 Over many years, they also experienced significant difficulties accessing effective services that accounted for gender identity and sexuality.193
In the absence of substantial research into effective treatment, at a minimum staff must have an awareness of the challenges faced by victim-survivors who identify as LGBTQIA+ and be adequately trained to meet their needs, either via their own services or effective collaboration. This is an area that warrants more attention from service providers in Tasmania.
- Male victim-survivors
We heard from many male victim-survivors of institutional child sexual abuse in Tasmania, such as Robert, who bravely reached out for help.
Robert’s experience
… here I was, 6 foot 6, walk into [the Sexual Assault Support Service], and I was standing behind a lady with her daughter and they moved on, and the lady behind the counter looked up at me and she said, ‘Oh, what do you want?’, and, yeah, at that time I broke down because it was … and I said, ‘I’m here, I’ve been sexually abused as a kid’, and she went, ‘Oh, oh’, and ran off and grabbed someone, but it was that kind of reaction of, you know, obviously they don’t get men or, you know, coming in all that often, let alone maybe sort of tall people that they would consider to be sort of strong enough to not go and get abused; yeah, everyone’s a kid at some stage, yeah. 194
Although overall, more females than males report child sexual abuse, there is still a substantial number of male victim-survivors who need to access the therapeutic service system.195 Evidence suggests that historically more males than females experienced child sexual abuse in an institutional setting.196
The National Royal Commission observed that male and female victim-survivors of child sexual abuse often have different needs, and so sexual assault services must consider the needs of males who seek their services.197 This could be particularly important for services set up to respond to gendered violence, where males are not immediately considered to be potential victim-survivors. The National Royal Commission heard that the greater number of female counsellors in sexual assault services can restrict males’ access to a male counsellor, which some would prefer.198
Therefore, it is important that male victim-survivors are included in the adult victim-survivors of child sexual abuse advisory group (refer to Recommendation 19.5 in Chapter 19) and that sexual assault services ensure they are set up to meet the needs of men and boys who seek help. Also, the Government must increase the visibility of sexual assault services as catering to male victim-survivors.
- Victim-survivors from culturally and linguistically diverse backgrounds
The National Royal Commission heard that people from culturally and linguistically diverse backgrounds face specific barriers to accessing appropriate services. These include:
- concerns around privacy, confidentiality and conflicts of interest in small communities
- inadequate cultural competence among practitioners, including lack of knowledge of culturally acceptable ways to discuss sex and sexuality
- racism and discrimination from service staff
- mainstream services offering individualised responses where community-based approaches may be more culturally appropriate
- multicultural organisations lacking training in child sexual abuse
- lack of appropriate referral pathways
- scarcity of interpreters able to work appropriately with victim-survivors who are independent of the victim-survivor’s community
- failure to provide culturally appropriate information about child sexual abuse and available services in different languages.199
We received limited information about victim-survivors from culturally and linguistically diverse backgrounds overall. In Hobart and Launceston, we contacted agencies that support culturally and linguistically diverse communities.200 We invited them to speak with us but, unfortunately, none provided information or attended stakeholder consultations.
However, given the findings of the National Royal Commission and our awareness of the needs of culturally and linguistically diverse people in Tasmania, we consider there is room for improvement in creating specialist sexual assault services for victim-survivors that can accommodate people from a variety of backgrounds in a culturally appropriate way, including greater collaboration. The National Royal Commission found that collaboration ‘is particularly important for meeting the needs of victims and survivors from culturally and linguistically diverse backgrounds’; this can mean integrating specialist culturally and linguistically diverse services into mainstream services or coordinating victim-survivors’ care in different parts of the service system.201
- Diversity and inclusion at Arch centres
All victim-survivors should have choices and be able to access the specialist knowledge that Arch centres are designed to provide. Therefore, it is essential that Arch centres respect diversity and inclusion.202 Laurel House Chief Executive Officer, Kathryn Fordyce, said that centres ‘should be welcoming and engaging for children and adults regardless of gender, sexuality, disability, cultural background and experience’.203 Tasmania Police Commissioner Hine indicated that:
… there will be services engaged to provide specialised advice and support who are not co-located but are within close proximity to the facility. These will include services specific to the individual needs of people with a disability, culturally diverse and indigenous cultural requirements.204
Given the centrality of collaboration to successful therapeutic care, it will be important for Arch centres to carefully consider how services directed at particular groups will work alongside those at the centres. It is not enough to engage specialist services; mainstream services must ‘have the skills and capability to respond effectively to diverse needs or collaborate with other agencies to meet those needs’.205
Recommendation 21.6
- The Tasmanian Government should ensure that the needs of particular groups of victim-survivors are met by the therapeutic service system and related contracting of services, including the needs of:
- children who are victim-survivors or have displayed harmful sexual behaviours (Recommendation 21.8)
- victim-survivors with disability or mental illness
- victim-survivors who identify as LGBTQIA+
- male victim-survivors
- victim-survivors who are from culturally and linguistically diverse backgrounds.
- The Tasmanian Government should consult on the therapeutic service system with relevant stakeholder groups, including the Interim Disability Commissioner, community groups and representative bodies.
- Aboriginal healing centres
The National Royal Commission recommended that federal, state and territory governments fund Aboriginal and Torres Strait Islander healing approaches as part of therapeutic services for victim-survivors of child sexual abuse.206 Despite this, in Tasmania there are no specific Aboriginal healing services for victim-survivors of child sexual abuse. The Tasmanian Aboriginal Centre provides some therapeutic services via programs such as its health services, family services and children’s services.207 While victim-survivors are generally supported to access mainstream sexual assault counselling services, the Tasmanian Aboriginal Centre also employs some practitioners ‘with specialist experience in sexual assault treatment’.208 Other Tasmanian Aboriginal organisations also support community members in various ways, including with healing from child sexual abuse, but do not have targeted programs.209
Heather Sculthorpe, Chief Executive Officer, Tasmanian Aboriginal Centre, told us that some of the barriers to providing Aboriginal healing services include inconsistent government funding as well as ‘narrowly targeted funding’ that does not ‘recognise the importance of ongoing relationships in the Aboriginal community’.210
Adding to this, our research found no evidence to suggest that existing sexual assault services have sought to specifically develop culturally appropriate approaches. This may create a barrier for Aboriginal people to access sexual assault services because they appear intrinsically ‘white’, and limit the effectiveness of counselling provided to those Aboriginal victim-survivors who do engage. Participants in one consultation told us that the ‘white’ way of counselling not only differs from but it also ‘undermines the First Nations approach’.211 One Aboriginal victim-survivor told us that support services consistently failed to take into account cultural identity, which compounded their trauma.212 We also heard that existing services do not necessarily have capacity: ‘when abuse happens, you need timely support—there is a waitlist for everything’.213
When we conducted consultations with Aboriginal communities, we frequently heard about the lack of culturally appropriate therapeutic services in Tasmania. We heard about the following service needs:
- Aboriginal-led therapeutic services across the State that encompass an understanding of intergenerational trauma and are genuinely designed and led by Aboriginal people:
It has to be authentic co-design, not Aboriginal people being asked afterwards … You need to listen to our ideas because our communities worked for thousands of years. The government is always trying to come up with these innovative things, but the knowledge is already sitting there in Aboriginal communities … Let us mend and fix our community.214
- Aboriginal-run cultural healing centres on Country across the State where children and families can visit or stay to receive support (this is also discussed in Chapter 9): ‘We need our kids to have a space where they can be with community members and still looked after’.215
- Training and development opportunities to support Aboriginal people to gain therapeutic skills to benefit their communities:
- Consistent funding for therapeutic programs, including those that are already working well. Organisations ‘have to have reliable funding, otherwise you are playing with people’s lives’.218
Given the over-representation of Aboriginal children in out of home care and in youth detention, and that harmful sexual behaviours often occur in those settings, these therapeutic programs also need to be equipped to address harmful sexual behaviours.
We heard that part of embedding culture is having programs that are Aboriginal-led and -controlled. Ms Sculthorpe stated that successful programs require ‘Aboriginal decision-making in the context of Aboriginal community control’.219 This approach is supported by the Healing Foundation, which, in response to the National Royal Commission, found that:
… a culturally based approach to understanding trauma and to resourcing healing and recovery is required by Aboriginal and Torres Strait Islander people who have been, or may in the future be, sexually abused in public and private institutions, and that healing is most effective when designed, developed and delivered by Aboriginal and Torres Strait Islander people with and for their own communities.220
In Chapter 9 on out of home care, we recommend establishing recognised Aboriginal organisations (Recommendation 9.15). We also recommend implementing all elements of the Aboriginal and Torres Strait Islander Child Placement Principle (Recommendation 9.15).221 This recommendation includes investing in Aboriginal-led targeted early intervention and prevention services, transferring decision-making authority to Aboriginal organisations and establishing therapeutic residential programs for Aboriginal children. There is also a need for Aboriginal-led healing programs to be established more widely.
We are pleased that the Tasmanian Government has recognised this service gap and has committed in Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027 to Aboriginal-led ‘deep collaboration’ with Aboriginal organisations to ‘agree actions and strategies to prevent and respond to family and sexual violence in the Aboriginal community’.222
Models for Aboriginal services can be found nationally and may be useful to inform programs in Tasmania. For example, alongside community members, the Healing Foundation has developed resources, such as a guide to establishing ‘healing centres’ and a training program for communities working with victim-survivors of child sexual abuse.223 The central tenets of these resources—such as strengthening connections to community and culture and emphasising design and implementation by and for Aboriginal people—are reflected in the ideas shared with us by local Aboriginal communities.224
It became apparent during our community consultations that the healing of Aboriginal victim-survivors is inextricably linked to colonisation and intergenerational trauma, as well as to cultural and family needs: ‘when something happens to someone in our mob, it affects all of us’.225 While this broader landscape extends beyond our terms of reference, we consider that to be effective and culturally appropriate, Aboriginal healing services developed for victim-survivors of child sexual abuse must be broad in scope and enabled to take a holistic approach.
Similarly, we heard from Aboriginal communities about how taxing it can be to be frequently ‘consulted’ by government, especially when consultation does not result in desired changes. One participant spoke about contributing to numerous consultation processes but never seeing change: ‘look where we are. I’m tired. I’m so tired’.226 In consultation processes, Aboriginal communities nationwide are generally ‘asked to do a lot of work, a lot of which is unpaid or un-resourced’.227 Consequently, developing existing and new healing services must be carefully planned, well-funded and Aboriginal-led to avoid unfairly adding to this burden.
In addition to Aboriginal-led healing approaches, existing sexual assault services should improve their cultural appropriateness for Aboriginal victim-survivors. For a variety of reasons, some Aboriginal people will prefer to seek support from non-Aboriginal-led services, so sexual assault services need to become more comfortable and effective for Aboriginal victim-survivors of institutional child sexual abuse. One important way of achieving this is to ensure these agencies have representation from Aboriginal communities on their boards of management or in their executive structures. In that way, sexual assault services would have an internal source of assistance to improve the cultural appropriateness of their services.
Recommendation 21.7
The Tasmanian Government should improve healing services for Aboriginal victim-survivors and their families and communities by:
- fully resourcing and supporting recognised Aboriginal organisations across the state to design, develop and deliver Aboriginal-led healing approaches targeted to victim-survivors of child sexual abuse
- ensuring Aboriginal representation on the boards of management or in the executive structures of sexual assault services.
- Strengthening services for children who have displayed harmful sexual behaviours
Terminology and definition
We have adopted the National Office of Child Safety National Clinical Reference Group’s draft definition of harmful sexual behaviours, which was proposed in December 2022, for general use across Australian jurisdictions:
Harmful sexual behaviours are sexual behaviours displayed by children and young people that fall outside what may be considered developmentally, socially, and culturally expected, may cause harm to themselves or others, and occur either face to face and/or via technology. When these behaviours involve another child or young person, they may include a lack of consent, reciprocity, mutuality, and involve the use of coercion, force, or a misuse of power.228
We note that the National Office for Child Safety is continuing to work with the National Harmful Sexual Behaviours Clinical Reference Group, states and territories to finalise a nationally endorsed definition of harmful sexual behaviours. This definition, when finalised, should inform the definition in the whole of government harmful sexual behaviours framework (Recommendation 21.8) and related Tasmanian Government documents, policies and practice guidance.
For the following reasons provided by harmful sexual behaviours researcher Dr Gemma McKibbin, we have also taken care with the use of the terms ‘victim’, ‘victim-survivor’ and ‘perpetrator’ in this section, in keeping with the general view of the sector that children who engage in harmful sexual behaviours need help and assistance:
The binary between victim and perpetrator in instances of harmful sexual behaviour is not always clear. For example, in situations of sibling sexual abuse that is, where two or more siblings engage in sexual behaviour with one another, the initiator of the behaviour can change, and one sibling can be the perpetrator in one instance and the victim in another. It is important to use person-centred language; this means that we talk about the problem behaviour and not the problem child. It is important that we do not use stigmatising language as this actually inhibits children from recovering from being sexually abusive. I always use the language ‘child or young person displaying harmful sexual behaviour’.
Perpetrator is not the right term to use in the context of children and young people who sexually harm because it is stigmatising and obfuscates the harm that children have often experienced themselves. I do tend to use the term ‘victim-survivor’ for children or young people who have been sexually harmed by other children or young people. However, in some cases of sibling sexual abuse, the victim may also be a child who sexually harms. Further, a child who sexually harms is likely to be a victim of abuse in their own right. In this way the victim/perpetrator binary does not hold in cases of harmful sexual behaviour and more sophisticated thinking is needed in this space that accounts for the complexity of victimisation experiences.229
For the purposes of highlighting the specific therapeutic needs of children who have engaged in harmful sexual behaviours, we have distinguished between children who have engaged in harmful sexual behaviours and those who have been subject to them. As mentioned, we have considered those children who have been subject to another’s harmful sexual behaviours as ‘victim-survivors’ in terms of their therapeutic needs—that is, they will likely require sexual assault counselling in the same way as other victim-survivors of child sexual abuse. But the distinction is somewhat artificial because many children who have engaged in harmful sexual behaviours are themselves victim-survivors of sexual abuse. Such children will need a therapeutic approach that addresses both their harmful sexual behaviours and their sexual abuse experiences. Therefore, it is common in other jurisdictions, as in Tasmania, for the harmful sexual behaviours service system to exist within the broader child sexual abuse therapeutic service system.
The National Royal Commission recognised that harmful sexual behaviours can have similar negative effects on a child as sexual abuse by an adult.230 Recognising the significance of the issue, the National Royal Commission dedicated an entire volume to the issue of harmful sexual behaviours.231 It made seven recommendations about harmful sexual behaviours in general, which required the Australian and state/territory governments to fund primary and secondary prevention strategies or services, and tertiary therapeutic services. In relation to harmful sexual behaviours, in summary, the National Royal Commission recommended that:
- support services be accessible for all children and young people, regardless of age, incarceration, voluntary status, disability, cultural background, gender, sexual orientation, geographic location, setting or the nature of the sexual behaviour
- support be increased for generalist counselling services to improve their responsiveness to harmful sexual behaviours
- therapeutic services be safe, developmentally appropriate, trauma-informed, culturally informed, have clear referral pathways and provide a systemic intervention, with good staff training and supervision
- therapeutic services be evaluated to ensure effectiveness.232
We heard of significant problems with how institutions responded to harmful sexual behaviours in schools, out of home care and Ashley Youth Detention Centre (refer to Chapters 5, 6, 8, 9, 11 and 12). These institutions appear to be the most at risk of harmful sexual behaviours occurring.233
A mother’s experience—the importance of timely intervention
A mother told us that her two primary-aged children were sexually abused by an older boy from school. They told her that he was coercive and violent. She described her children’s traumatised responses of incontinence, emotional outbursts, self-harm and drawing sexual pictures.
Both children have disability, and the mother expressed fear for their mental health because they have told her they should kill themselves. She has experienced difficulty accessing timely and affordable services for them.
The older boy who displayed harmful sexual behaviours also has disability and has experienced violence in his home. The mother said she felt sorry for the boy, but she described the frustration of knowing that other parents had raised concerns about the older boy displaying harmful sexual behaviours before her, but the school took a long time to act, even after her complaint.
The mother said the school, because of privacy reasons, would not tell her if the boy was getting therapeutic help. She felt powerless to protect her children, so she changed schools, but she is worried for other students.234
- Understanding harmful sexual behaviours
Understanding harmful sexual behaviours and how to address these behaviours effectively is a rapidly developing field. Most frameworks consider the behaviours as occurring along a continuum of increasing deviation from what is considered normal for a child’s developmental age in terms of severity, duration and impact.235 They also consider that children engage in harmful sexual behaviours for a combination of reasons; these reasons are often called ‘pathways’ to harmful sexual behaviours.236
Due to this variation in severity and motivation, not all children who have engaged in harmful sexual behaviours will benefit from the same form of therapeutic intervention, and responses to harmful sexual behaviours need to be ‘both proportionate and appropriate’.237 For example, for less severe incidents that are motivated by misguided curiosity about sex, setting boundaries and educating about consent and appropriate behaviours are likely to be sufficient interventions to prevent a child engaging in those behaviours again.238 However, the more severe and persistent the behaviour, the more likely a child will need a more intensive specialised therapeutic response. Often criminal justice and child protection responses are also involved, depending on the circumstances of the behaviour.239 If the behaviour has occurred in youth detention or in an out of home care or school environment, those settings also will need to be involved in the response.
While research has shown that most adult sex offenders started their offending as teenagers, experts in harmful sexual behaviour interventions generally agree that therapeutic intervention for most children who engage in harmful sexual behaviours is effective in stopping the behaviours.240
Therefore, early intervention to address harmful sexual behaviours is paramount to prevent recurrence and minimise harm.241 Therapeutic intervention for harmful sexual behaviours requires specialist skills and training in addition to that required for counselling for child sexual abuse.242
In terms of the intensive specialised response required for children who have displayed behaviours further along the spectrum, recent literature reviews indicate that evidence for using any of the main approaches across a variety of settings is still being established.243 The experts we heard from suggested that several approaches could be effective when responding to harmful sexual behaviours.244 Rather than recommending a particular model, Dale Tolliday, a harmful sexual behaviours clinician, recommends that the Tasmanian Government adopts ‘best practice principles for therapeutic intervention for children with harmful sexual behaviours, which are relevant to children of all ages’, as identified by the National Royal Commission.245 Mr Tolliday and researcher, Dr Gemma McKibbin, recommended that therapeutic interventions should have certain key characteristics, which we have consolidated and summarised. Interventions should:
- be accessible to all children with harmful sexual behaviours and delivered early
- be based on an individual assessment of each child, with tailored therapy that takes a contextual and systemic approach, recognising other problems in the child’s life
- be safe, including through being non-punitive, trauma-informed and culturally safe
- assign accountability and responsibility for the harmful sexual behaviours
- focus on behavioural change and work towards broader outcomes than simply reducing harmful sexual behaviours
- use developmentally and cognitively appropriate interventions based on techniques that are specialised for treating harmful sexual behaviours
- be delivered by staff who have specialist training and supervision
- actively involve the parent or caregiver to support treatment.246
Mr Tolliday recommended that in developing its approach the Government considers these characteristics, as well as ensuring the model is suited to the way services are organised.247
In keeping with the National Royal Commission’s findings, Mr Tolliday said specialist harmful sexual behaviours treatment should sit within a broader public health approach to improve knowledge about harmful sexual behaviours and how to respond to them:
In particular, building service system capacity should include key general and focused prevention actions (primary and secondary prevention), building generalist service capacity to respond (such as schools, GPs, childcare services, child and youth counselling) as well as specialist services. Building only a specialist service limits [the] response to a limited number of children and families and the scale and scope of [problematic and harmful sexual behaviours] demands a larger and more comprehensive strategy.248
We agree.
- The Tasmanian Government’s response
The Department of Communities stated that the Government had responded to the National Royal Commission’s recommendations by:
- contributing to and signing on to the National Strategy to Prevent and Respond to Child Sexual Abuse 2021–2030 (released on 27 October 2021)
- funding the Sexual Assault Support Service for two years from 1 April 2021 to provide a statewide therapeutic program for children with harmful sexual behaviours (called Prevention, Assessment, Support and Treatment, discussed in Section 5.2.1), which the then Department of Communities said fulfils the principles in the National Royal Commission’s Recommendation 10.5
- funding the Sexual Assault Support Service for two years from 1 April 2021 to provide primary and secondary prevention programs for children engaging in problematic sexual behaviours (under the Prevention, Assessment, Support and Treatment program)
- funding an independent evaluation of the Sexual Assault Support Service’s Prevention, Assessment, Support and Treatment program for harmful sexual behaviours
- the Department of Justice representing Tasmania on the Inter-jurisdictional Working Group on Therapeutic Responses for Children with Problematic and Harmful Sexual Behaviours.249
Apart from contributing to the two national initiatives, the Tasmanian Government’s primary response to the National Royal Commission’s recommendations about harmful sexual behaviours is to fund a non-government organisation (the Sexual Assault Support Service) to deliver the Prevention, Assessment, Support and Treatment program.
While recognising the outstanding efforts of the Sexual Assault Support Service in identifying a service gap and attempting to fill it, we are concerned that this approach is not enough, which we discuss in Section 5.4.
- Prevention, Assessment, Support and Treatment program
Before April 2021, as part of their normal service delivery, Laurel House and the Sexual Assault Support Service provided interventions for children up to age 11 or 12 who had displayed harmful sexual behaviours.250
In April 2021, the Sexual Assault Support Service received government funding to provide a free, statewide specialist harmful sexual behaviours prevention and therapeutic intervention program for children up to 17 years of age—the Prevention, Assessment, Support and Treatment program.251 Laurel House also said it will still see children under 12 who have displayed harmful sexual behaviours in northern Tasmania and the North West, but it is not specifically funded for that work.252 Victim-survivors of harmful sexual behaviours can access supports through the Sexual Assault Support Service’s and Laurel House’s usual sexual assault counselling services.
The prevention and early intervention element of the Prevention, Assessment, Support and Treatment program involves the Sexual Assault Support Service presenting training sessions for school staff, Child Safety Service staff and other community members about how to prevent harmful sexual behaviours and respond to them appropriately if they occur.253 The service also presents sessions in primary and high schools about consent and respectful relationships that complement the sessions with school staff.254
We consider that the funding for this aspect of the Prevention, Assessment, Support and Treatment program is insufficient. The program is funded to provide the full set of harmful sexual behaviours awareness and response sessions to only four schools per year, although the Department for Education, Children and Young People funds another four.255 Other schools can purchase the training from the Sexual Assault Support Service.256 We calculate that, without schools purchasing the training themselves, it would take the Sexual Assault Support Service about 24 years to present government funded harmful sexual behaviours sessions to all 195 government schools in Tasmania.257 In Chapter 6, we recommend mandatory child sexual abuse prevention education in all schools.
The therapeutic element of the Prevention, Assessment, Support and Treatment program is funded for one specialist harmful sexual behaviours counsellor to work three days a week in each region: southern Tasmania, northern Tasmania and the North West.258 Mission Australia delivers case management for families alongside the Sexual Assault Support Service’s therapeutic intervention to assist with other issues that are assessed as contributing to the behaviours—for example, assisting to gain access to National Disability Insurance Scheme supports for a child with disability whose needs are not being appropriately addressed.259
Initially the program was funded for two years as a pilot, but Action 28 of Survivors at the Centre: Tasmania’s Third Family and Sexual Violence Action Plan 2022–2027 states that the Government will ‘continue to deliver’ the program.260 Although Action 28 lacks detail, we hope this means the program will be funded on an ongoing basis.261
In the year following the start of the program in April 2021, the Sexual Assault Support Service said it received 90 referrals for children who had displayed harmful sexual behaviours.262 Many of the referrals were from schools, parents and the Child Safety Service.263 As of 31 March 2022, the program had 29 active clients engaged with a therapist and an average waiting list of 10 children, who can wait from four-to-10 weeks for therapy.264
Despite the recent introduction of this therapeutic service for harmful sexual behaviours, we heard in submissions and at consultations that some people are still concerned about a lack of available therapeutic services in Tasmania for children exhibiting harmful sexual behaviours.265 Renae Pepper from the Sexual Assault Support Service told us that they have not actively promoted the Prevention, Assessment, Support and Treatment
program due to limited funding and said there have been plenty of referrals since starting the program; promotion would only exacerbate waiting lists.266
We consider that although funding the Prevention, Assessment, Support and Treatment program is a welcome start, the Government needs to increase the capacity of the therapeutic component of the service system’s response to harmful sexual behaviours. In addition, for all the reasons outlined above in relation to appropriate sexual assault services, these therapeutic services need to be designed to meet the needs of particular groups of children, including those with disability, who identify as LGBTQIA+, who are from a culturally or linguistically diverse background, or who are Aboriginal. It should be accessible to children statewide.
- Government agency responses
School-based responses
The Department for Education, Children and Young People has initiated its own response to the issue of harmful sexual behaviours among students in Tasmanian schools, including a flowchart to guide principals’ responses, a working group focused on the issue and appointing extra senior support staff.267 Timothy Bullard, Secretary of the Department, told us that the Department had received extra funding in the
2021–22 State Budget to equip staff to identify and respond to harmful sexual behaviours in schools.268
The Department’s approach appears to be based on the same model of understanding harmful sexual behaviours as the Sexual Assault Support Service has used for the Prevention, Assessment, Support and Treatment program: Hackett’s continuum of harmful sexual behaviours.269 We anticipate that by using the same model and linking its response to the Prevention, Assessment, Support and Treatment program, the Department can develop a common understanding of harmful sexual behaviours and the roles of schools and Prevention, Assessment, Support and Treatment therapists when coordinating a response.270
Unfortunately, the Department’s response for schools is not replicated elsewhere in Tasmanian Government institutions, because other areas that are often involved with children who have engaged in harmful sexual behaviours have not taken similar steps to improve their understanding of, or response to, harmful sexual behaviours.
Child protection responses
Many professionals and government employees are mandatory reporters and will advise the Advice and Referral Line of concerns about a child who has displayed harmful sexual behaviours. Concerned parties will also contact the Advice and Referral Line for advice and referral for a child’s sexualised behaviours.
The National Royal Commission considered that a child protection response to harmful sexual behaviours (in Tasmania this would involve the Advice and Referral Line referring the matter to the Child Safety Service) is generally only appropriate where other children are at risk and there is no parent who can act protectively.271
However, the need for protection is not always immediately clear. While the child’s behaviour may imply a risk to other children, research indicates that children who have engaged in harmful sexual behaviours may themselves be at risk of harm and in need of care and protection.272 Consequently, staff taking calls at the Advice and Referral Line need to have a nuanced understanding of, and ability to enquire into, the circumstances of an incident of harmful sexual behaviours.
Despite this, we heard evidence that suggested Advice and Referral Line staff were not always knowledgeable enough about responding to harmful sexual behaviours, particularly in institutional settings.
In Chapter 8 on out of home care, we report the results of our analysis of the files of 22 children in out of home care and note that Child Safety Officers did appear to refer children for specialist harmful sexual behaviour interventions. However, at our consultation with out of home care providers, they suggested that this is not consistently the case.273 They also considered that the Child Safety Service relied too heavily on Tasmania Police to respond to instances of harmful sexual behaviours.274 Given that out of home care is a high-risk institutional environment for children experiencing harmful sexual behaviours, we identify in Chapter 9 that the Child Safety Service and out of home care providers, carers and volunteers should be supported to build their knowledge and skills concerning harmful sexual behaviours.275
As established in Chapter 9, the Advice and Referral Line and the Child Safety Service receive little mandatory specialised training in child sexual abuse or harmful sexual behaviours, nor do they have a clear policy to guide staff when assessing and responding to harmful sexual behaviours.276 The only real direction provided to the Advice and Referral Line staff by the Child Safety Service is the Assessing and Responding to Sexual Abuse Procedure.277 The procedure instructs Advice and Referral Line staff to record a contact about a child’s harmful sexual behaviours in the Child Advice and Referral Digital Interface and—if the child is 10 years of age or older—to record it as an ‘incident’ in the Child Protection Information System.278 In some circumstances, the procedure suggests the Advice and Referral Line may refer a concern about a child who has engaged in harmful sexual behaviours to the Child Safety Service for assessment and/or to police, although the procedure is not clear about when this might occur.279
We are not confident that Advice and Referral Line staff have been supported with the skills and knowledge to ensure children who have engaged in harmful sexual behaviours or who are victim-survivors of harmful sexual behaviours are protected, as well as referred for appropriate therapeutic supports. The Government should address this gap in developing a whole of government framework to address harmful sexual behaviours and in drafting detailed and specific out of home care policies, protocols and practice guidance to support best responses to harmful sexual behaviours displayed or experienced in out of home care (Recommendation 9.28). There should also be mandatory induction and ongoing professional development about child sexual abuse and harmful sexual behaviours, as well as policy guidance and access to the Harmful Sexual Behaviours Support Unit for assistance (refer to Recommendation 9.28).
Criminal justice responses
A criminal justice response will be relevant only for a minority of harmful sexual behaviours that meet the criteria for a potential criminal offence. These cases require that the child displaying the behaviours is old enough to be considered to have criminal responsibility for their actions under the law and for the behaviour itself to amount to the physical element of a criminal offence.280 However, Tasmania Police will often need to be involved in a case of harmful sexual behaviours to determine if the behaviour meets the threshold for charges to be laid, and if there is enough evidence for a charge.
Police may receive a report about a child who has engaged in harmful sexual behaviours from the Advice and Referral Line, the Child Safety Service, a school or from a parent.281 Our analysis of the 22 files of children in out of home care, set out in Chapter 8, confirmed that Tasmania Police and the Child Safety Service regularly refer incidents of harmful sexual behaviours to each other.
However, the Sexual Assault Support Service expressed concern about the coordination of referrals from Tasmania Police for therapeutic support services for victim-survivors of harmful sexual behaviours.282 It said the service receives very few referrals for harmful sexual behaviours from police and that those they do receive may be inaccurate—for example, when a child is referred for harmful sexual behaviours, but upon inquiry the case is clearly one of child sexual exploitation.283
When deciding on a response, Tasmania Police indicated a preference for diversion in instances of harmful sexual behaviours.284 We agree. But we acknowledge that there will be some children detained in youth justice due to engaging in sexual violence. In Chapter 16, we discuss the usefulness of a therapeutic component forming part of youth justice options for children who have been charged with or convicted of a sexual offence, using the court’s diversionary powers.
The Keeping Children Safe Handbook outlines how Tasmania Police and the Child Safety Service will interact in response to child protection concerns.285 Unfortunately, the handbook offers minimal direction to either agency in how to respond to harmful sexual behaviours, outside of referring one to the other in circumstances ‘where a child is an alleged offender’.286
The use of terms such as ‘alleged offender’ or ‘alleged perpetrator’ are commonplace law enforcement terms. However, as discussed in ‘Terminology and definition’ above, such language stigmatises children who have displayed harmful sexual behaviours and can interfere with providing a trauma-informed response and therapeutic intervention.
To improve the effective response by Tasmania Police and the Child Safety Service to harmful sexual behaviours, the Keeping Children Safe Handbook should be updated to include clear directions that are trauma-informed and use language that reflects modern understandings of harmful sexual behaviours. Having shared definitions and understandings of harmful sexual behaviours will also help achieve a consistent response to this behaviour across government agencies.
- Involuntary treatment
Jenny Wing, Chair of the peak body Victorian Harmful Sexual Behaviour Network, told us that most children who receive therapeutic interventions in the Victorian Sexually Abusive Behaviour Treatment Services do so voluntarily.287 However, occasionally a family and/or their child will not consent to treatment, thus placing other children and the child themselves at more risk because the concerning behaviour goes unaddressed.288
If the Child Safety Service decides that a child does not need care and protection and the matter is not pursued by police, it can be difficult to impose interventions without parental agreement.289 The National Royal Commission identified that ‘in most states and territories, there is no express legal basis upon which child protection agencies can respond’.290 The exception would be if it can be proven that the child is at risk of abuse or harm as required by the Children, Young Persons and Their Families Act 1997.291
Dale Tolliday, the harmful sexual behaviours treatment expert previously mentioned, told us that compulsory treatment for harmful sexual behaviours can be necessary, but should be a last resort:
[Treatment] should be therapeutic rather than punitive. More coercive strategies may be required for more serious and/or repeat cases, or where engagement strategies fail, but effectively dealing with these behaviours early on is the best form of prevention.292
Where the child is not facing criminal charges for the harmful sexual behaviours, there is a need for a mechanism that would allow children with harmful sexual behaviours to be treated when parents or carers are unwilling to engage voluntarily.
The most logical way would be to amend the Children, Young Persons and Their Families Act 1997 to provide an explicit legislative power to allow the Magistrates Court (Children’s Division) to order a child to receive therapeutic intervention for harmful
sexual behaviours. This has been done successfully in Victoria with the introduction of therapeutic treatment orders and would empower the Child Safety Service to protect the child and other children in the complex context of harmful sexual behaviours.293
In Victoria, if a child appears before the Criminal Division of the Children’s Court on a criminal charge and the court considers there are grounds to apply for a therapeutic treatment order in respect of the child, the Court can refer the matter to the Secretary of the Victorian Department of Families, Fairness and Housing for investigation.294 In deciding whether to refer a matter to the Secretary, the Court must consider the seriousness of the child’s sexually abusive behaviours, among other matters.295
If, on the application of the Secretary, the Family Division of the Children’s Court makes a therapeutic treatment order in respect of the child, the Criminal Division must adjourn the criminal proceedings to enable the child to complete the therapeutic treatment order.296 Once the child has completed the order, and the Criminal Division is satisfied that the child has attended and taken part in the therapeutic treatment program, the Court must discharge the child without any further hearing of the criminal proceedings.297 We recommend that Tasmania adopts a similar mechanism (refer to Chapter 16).
The introduction of therapeutic treatment orders in Victoria has delivered secondary, and possibly more important, consequences for children with harmful sexual behaviours. Ms Wing observed better collaboration between statutory child protection, police, children’s courts and the sexual abuse behaviour treatment services, as well as increased confidence in the effectiveness of harmful sexual behaviour interventions.298
- A broader whole of government response
We are concerned that the Government’s principal response to the issue of harmful sexual behaviours in Tasmania has been to fund a non-government organisation to provide a limited range of prevention and intervention services that does not meet demand. Apart from the Department for Education, Children and Young People’s decision to improve its response to harmful sexual behaviours to align with the Prevention, Assessment, Support and Treatment program, the Government does not have a consistent response across agencies. This is far from sufficient to address the National Royal Commission’s recommendations or, more importantly, to meet the needs of children who have displayed harmful sexual behaviours.
Other jurisdictions are working to standardise responses to harmful sexual behaviours, such as New South Wales’ Children First 2022–2031 shared whole of government framework for preventing and responding to problematic and harmful sexual behaviours by children and young people, which provides a sector-wide, multiagency public health approach.299
Other examples include Western Australia’s Understanding and Guiding Responses to Harmful Sexual Behaviours in Children and Young People and South Australia’s work towards an ‘interagency response framework’, which is underway with the University of South Australia (projects in which Commissioner Bromfield is involved).300
The Victorian Government has also developed a framework to respond to harmful sexual behaviours that includes prevention, early intervention and therapeutic intervention.301 The Victorian Government has funded sexual abuse behaviour treatment services across the State since the early 2000s, which it ‘attached’ to its existing network of government funded non-government organisations that deliver specialist sexual trauma services across Victoria.302 Ms Wing told us that the Victorian model of assigning harmful sexual behaviours services to geographical regions creates a more cooperative and better quality service system because it avoids the ‘hostile environment’ that can develop between agencies when funding is competitive.303
Ms Wing identified several advantages to harmful sexual behaviour interventions being delivered as part of the sexual assault service system, including harnessing existing expertise in child sexual abuse and the ability to adapt to local contexts.304
In addition to increasing the availability and accessibility of therapeutic services for children who have engaged in harmful sexual behaviours, the Tasmanian Government must also lead a whole of government response to harmful sexual behaviours. Undertaking this task will assist government agencies that have the greatest involvement with children who have displayed harmful sexual behaviours to be equipped to prevent and respond to the issue. The response must be coordinated across departments, which requires a common understanding of the issue and an agreed approach between departments and the therapeutic service system for harmful sexual behaviours.
The Tasmanian Government should develop a statewide framework for preventing, identifying and responding to harmful sexual behaviours. The framework should provide a common understanding of harmful sexual behaviours, high-level guidance on how to respond, and clear roles and responsibilities of different government provided and funded agencies in the response. The definition adopted in the framework should be informed by the work of the National Office for Child Safety in developing a revised national definition for harmful sexual behaviours.
In developing the framework, the Tasmanian Government should carefully consider when and for what purpose incidents of harmful sexual behaviours in government institutions should be reported to Tasmania Police and the Advice and Referral Line. This should consider the role of these agencies in responding to harmful sexual behaviours, different responses for children under and over the age of criminal responsibility, and the intention for harmful sexual behaviours to be responded to with diversionary and therapeutic responses in the first instance.
The Government should develop the framework in consultation with stakeholders and include the role of government funded services that form part of the State’s harmful sexual behaviour response, such as the Prevention, Assessment, Support and Treatment program.
Services for children displaying harmful sexual behaviours should be considered in the Arch centres. We heard that such services are often co-located in multidisciplinary centres in Victoria, which facilitates collaboration and provides an advantage when dealing with in-family harmful sexual behaviours, because both the child who has experienced harmful sexual behaviours and the child who has displayed harmful sexual behaviours are seen in one location.305 This means families do not need to ‘tell their story multiple times’ and staff develop ‘a more sophisticated understanding of the dynamics of sexual violence’.306 This practice would be possible at Arch centres.
The framework should be translated into action through detailed context-specific policies, protocols and guidance, including those we have recommended for education, out of home care and youth justice (refer to Recommendations 6.9, 9.28 and 12.30). We have identified several existing statewide frameworks developed for other jurisdictions above. While we do not recommend a particular framework, we note that the authors of these approaches appear to be open to making their work available and have made materials publicly available.307 The Department would likely find it cost-effective to adapt material from existing approaches to the Tasmanian context.
Recommendation 21.8
- The Tasmanian Government, in collaboration with key stakeholders, should develop a statewide framework and plan for preventing, identifying and responding to harmful sexual behaviours. The framework should:
- agree on a common definition and understanding of harmful sexual behaviours, including adopting a recognised, contemporary continuum of sexual behaviours from ‘developmentally expected’ to ‘harmful’
- use an evidence-informed framework for understanding, preventing, identifying and responding to harmful sexual behaviours
- clarify the roles and responsibilities of the various agencies and departments involved in preventing and responding to the full continuum of harmful sexual behaviours, including programs delivered by non-government providers
- meet the needs of particular groups of children (Recommendation 21.6)
- include structures to support ongoing engagement with emerging evidence regarding harmful sexual behaviours
- include an evaluation framework.
- The Tasmanian Government should ensure the therapeutic service system for children who have displayed harmful sexual behaviours:
- provides sufficient therapeutic services that can be accessed in a timely manner
- ensures timely access to therapeutic services for all children who need them, regardless of their age, identity or location in the state (including in youth detention)
- ensures specialist interventions for children with disability
- ensures all providers of therapeutic interventions for harmful sexual behaviours have Aboriginal representation in their governance structure.
- The Tasmanian Government should provide ongoing and increased funding for specialist therapeutic interventions for harmful sexual behaviours that:
- ensures children who have displayed abusive or violent harmful sexual behaviours and their families need not wait more than two weeks for support when therapeutic treatment is required
- provides an advisory service for child-facing organisations, such as independent schools, childcare, disability and at-risk youth services and Tasmania Police (this service is not intended for the Department for Education, Children and Young People, which will have access to an internal Harmful Sexual Behaviours Support Unit (Recommendation 9.28))
- contributes to the statewide plan for preventing harmful sexual behaviours and its agencies’ responses to children who have displayed such behaviours.
Recommendation 21.9
The Tasmanian Government should introduce legislation to amend the Children, Young Persons and Their Families Act 1997 and the Youth Justice Act 1997 to:
- give the Magistrates Court explicit power to order that a child who has displayed harmful sexual behaviours (and their family) engage in a therapeutic intervention for harmful sexual behaviours
- ensure the Magistrates Court has the power to divert from the criminal justice system a child who has been charged with a criminal offence and who has engaged in harmful sexual behaviours, by adjourning the criminal proceeding to enable the child to engage in a therapeutic intervention, and discharging the child where the intervention has been completed successfully.
Recommendation 21.10
Tasmania Police and the Department for Education, Children and Young People should update the Keeping Children Safe Handbook to reflect the Tasmanian Government’s statewide framework and plan for addressing harmful sexual behaviours, including by:
- modifying the language used when discussing children who have displayed harmful sexual behaviours to align with the definitions developed through the National Office of Child Safety
- clarifying the roles and responsibilities of the two agencies in responding to incidents involving harmful sexual behaviours, including the conditions under which each agency will lead the response
- clarifying the involvement of specialist therapeutic services in responses to incidents.
- Conclusion
Our Inquiry into Tasmania’s therapeutic service system for victim-survivors of institutional child sexual abuse and children who have displayed harmful sexual behaviours has revealed scope for improvement.
Specialist services for victim-survivors are few and staffed by hard-working, dedicated professionals who have advocated for increased services and better coordination for many years. Even after the National Royal Commission made many recommendations to create a responsive service system for victim-survivors, the Tasmanian Government has continued to adopt a passive position of responding with piecemeal funding offerings instead of assuming leadership for providing a robust service system.
It is vital that the Tasmanian Government leads the development and funding of a responsive service system. The Government must ensure services reach those who are missing out, such as children in Ashley Youth Detention Centre, victim-survivors with disability, victim-survivors who identify as LGBTQIA+, victim-survivors from culturally and linguistically diverse backgrounds, male victim-survivors and those in isolated communities or Aboriginal victim-survivors.
For children who have displayed harmful sexual behaviours, the Tasmanian Government has only recently responded to the National Royal Commission’s recommendations by funding a single service to provide services across the State. This is not enough, and it lacks the government leadership required to provide a collaborative, effective therapeutic service system for children who have these difficulties. The Tasmanian Government should develop a cross-agency framework to prevent and respond to harmful sexual behaviours.
Notes
1 Statement of Michael Salter, 7 April 2022, 31 [120]–32 [121].
2 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 143 [22]–144 [9].
5 Department of Justice, Fifth Annual Progress Report and Action Plan 2023 (Report, December 2022).
12 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 142 [32–33].
13 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 135 [1–12].
15 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 134 [38]–135 [12].
16 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 135 [3–7].
18 Submission 069 Laurel House, 5; Submission 073 Sexual Assault Support Service, 3.
21 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 135 [19–29], 142 [20–33].
22 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 137 [35–39], 142 [27–33].
23 Statement of Jillian Maxwell, 26 April 2022, 2 [11].
24 Laurel House, Annual Report 2021 (Report, 2021) 14–16.
26 Session with Keelie McMahon, 13 March 2022.
32 Submission 069 Laurel House, 5.
35 Statement of Kathryn Fordyce, 3 May 2022, 11 [31].
36 Statement of Kathryn Fordyce, 3 May 2022, 11 [31–35].
38 Statement of Catherine Edwards, 7 April 2022, 3 [14].
39 Statement of Catherine Edwards, 7 April 2022, 13 [89].
41 1800RESPECT National Sexual Assault Domestic Family Violence Counselling Service, Homepage (Web Page, 2022) <https://www.1800respect.org.au/>.
45 Statement of Kathrine Morgan-Wicks, 24 May 2022, 19 [162].
52 Notice to produce served on the State of Tasmania, 20 July 2021, 2–3. to produce served on the State of Tasmania, 20 July 2021, 2–3.
55 Submission 073 Sexual Assault Support Service, 20.
57 Session with Kylee Pearn, 5 October 2021.
60 Consultation with Burnie community, 24 August 2021.
61 Statement of Kathryn Fordyce, 3 May 2022, 14 [44].
62 Submission 087 Anonymous, 1, 3.
63 Statement of Jillian Maxwell, 26 April 2022, 5 [28], 7 [38].
81 Statement of Jennifer Wing, 8 June 2022, 16 [66].
82 Statement of Peter Yeomans, 24 April 2022, 6 [30].
84 Transcript of Darren Hine, 6 July 2022, 2471 [10–16].
86 Transcript of Darren Hine, 6 July 2022, 2479 [18–24].
87 Statement of Kathryn Fordyce, 3 May 2022, 14 [44].
91 Victoria Police, Victoria Police Procedural Fairness Response, 10 March 2023, 1.
93 Statement of Darren Hine, 14 June 2022, 25 [110].
95 Statement of Jonathan Higgins, 8 August 2022, 25 [83].
96 Statement of Darren Hine, 14 June 2022, 33 [138].
98 Transcript of Jillian Maxwell, 3 May 2022, 153 [30-33].
101 Statement of Darren Hine, 14 June 2022, 50 [192].
103 Submission 073 Sexual Assault Support Service 13–14.
111 Statement of Jenny Wing, 8 June 2022, 3 [13–14].
112 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 143 [45]–144 [9].
113 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 143 [45]–144 [9].
115 Session with Angelique Knight, 17 March 2022; Session with Keelie McMahon, 16 March 2022.
116 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 137 [41–45].
117 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 141 [24–25], 142 [22–27].
119 Submission 039 Dianne Calderbank, 5.
120 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 137 [32–33], 142 [9–13].
122 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 135 [42]–136 [29], 143 [3–11].
123 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 145 [17–45].
126 Session with Angelique Knight, 17 March 2022; Statement of Keelie McMahon, 31 May 2022, 6 [31].
127 Statement of Catherine Edwards, 4 July 2022, 9 [58].
128 Statement of Catherine Edwards, 4 July 2022, 4 [28].
129 Transcript of Catherine Edwards, 7 July 2022, 2582 [15–20].
130 Transcript of Catherine Edwards, 7 July 2022, 2583 [33–37].
132 Statement by Michael Salter, 7 April 2022, 33 [130].
133 Consultation with Queenstown community, 27 August 2021.
134 Consultation with Aboriginal community members, North West Tasmania, 28 September 2022.
137 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 139 [44]–140 [6].
138 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 138 [39]–139 [16].
139 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 139 [4–6].
140 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 140 [16–18].
141 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 140 [12–19].
142 Consultation with Queenstown community, 27 August 2021.
143 Transcript of Darren Hine, 6 July 2022, 2472 [39–42].
144 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 139 [11–14], 140 [2–12].
145 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 152 [13–18].
146 Statement of Jillian Maxwell, 26 April 2022, 14 [75].
147 Order of the Commission of Inquiry, restricted publication order, 16 June 2022.
148 Statement of Azra Beach, 14 June 2022, 7 [40–41].
149 Refer to the Glossary for a definition of ‘trauma-informed’.
150 Correspondence from Michael Pervan to Leanne McLean, 16 June 2022.
151 Statement of Renae Pepper, 30 April 2022, 17-18 [72].
152 Transcript of Vincenzo Caltabiano and Hannah Phillips, 19 August 2022, 2900 [41]–2901 [13].
155 Statement of Jillian Maxwell, 26 April 2022, 10 [59].
156 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 148 [11–22].
157 Statement of Michael Pervan, 28 July 2022, 88 [357], 92 [380].
158 Statement of Michael Pervan, 28 July 2022, 93 [386].
159 Submission 068 Care Leavers Australasia Network, 2, 8.
160 Submission 068 Care Leavers Australasia Network, 8.
161 Anonymous session, 30 March 2022.
168 Submission 073 Sexual Assault Support Service, 4.
172 Statement of Sally Robinson, 26 April 2022, 5 [16]–6 [19].
173 Statement of Sally Robinson, 26 April 2022, 6 [21].
174 Statement of Sally Robinson, 26 April 2022, 6 [23]–10 [37].
178 Statement of Dale Tolliday, 29 April 2022, 4 [16(e)].
179 Stakeholder consultation with non-government out of home care providers, 25 October 2021.
180 Statement of Sally Robinson, 26 April 2022, 24 [99], 25 [104].
182 Statement of Sally Robinson, 26 April 2022, 24 [99]–27 [113].
183 Statement of Sally Robinson, 26 April 2022, 24 [99]–29 [124].
185 Laurel House Sexual Assault Support, Disability Workforce Support Toolkit and Resources (Web Page, 2023) <https://laurelhouse.org.au/get-educated/disability-workforce-support-project/>.
189 Statement of Xris Reardon, 4 May 2022, 7 [28]-8 [33], 9 [37], 15 [66].
190 Statement of Xris Reardon, 4 May 2022, 9 [37], 10 [42].
191 Anonymous session, 8 June 2022.
194 Transcript of Robert Boost, 12 September 2022, 3892 [1–12].
203 Statement of Kathryn Fordyce, 3 May 2022, 14 [44].
204 Statement of Darren Hine, 14 June 2022, 50 [191].
207 Tasmanian Aboriginal Centre, Health (Web Page, 2023) <http://tacinc.com.au/programs/health/>.
208 Statement of Heather Sculthorpe, 15 June 22, 7.
210 Statement of Heather Sculthorpe, 15 June 22, 6.
211 Consultation with Aboriginal community members, southern Tasmania, 21 February 2023.
212 Submission 142 Anonymous, 2.
214 Consultation with Aboriginal community members, southern Tasmania, 24 October 2022.
215 Consultation with Aboriginal community members, southern Tasmania, 22 February 2023.
216 Consultation with Aboriginal community members, southern Tasmania, 22 February 2023.
217 Consultation with Aboriginal community members, North West Tasmania, 8 April 2022.
218 Consultation with Aboriginal community members, northern Tasmania, 18 July 2022.
219 Statement of Heather Sculthorpe, 15 June 22, 12.
220 Statement of Richard Weston, 10 June 2022, 16 [61].
223 Statement of Richard Weston, 10 June 2022, 11 [40], 18 [68].
224 Statement of Richard Weston, 10 June 2022, 17-18 [66].
225 Consultation with Aboriginal community members, southern Tasmania, 22 February 2023.
226 Consultation with Aboriginal community members, southern Tasmania, 22 February 2023.
227 Statement of Richard Weston, 10 June 2022, 6 [23].
229 Statement of Gemma McKibbin, 6 May 2022, 5 [14].
234 Anonymous session, 12 October 2022.
237 Statement of Gemma McKibbin, 6 May 2022, 14 [47].
238 Statement of Gemma McKibbin, 6 May 2022, 11 [35].
244 Statement of Dale Tolliday, 29 April 2022, 13 [55–56].
247 Statement of Dale Tolliday, 29 April 2022, 15 [65]–16 [69].
248 Statement of Dale Tolliday, 29 April 2022, 17 [71].
251 Statement of Renae Pepper, 30 April 2022, 4 [16].
252 Transcript of Jillian Maxwell and Kathryn Fordyce, 3 May 2022, 158 [3–15].
254 Statement of Renae Pepper, 30 April 2022, 5 [21].
255 Transcript of Renae Pepper, 10 May 2022, 728 [22–33].
256 Statement of Renae Pepper, 30 April 2022, 3 [14].
258 Transcript of Renae Pepper, 10 May 2022, 730 [1–18].
259 Transcript of Renae Pepper, 10 May 2022, 725 [1–8].
262 Statement of Renae Pepper, 30 April 2022, 8 [34].
264 Statement of Renae Pepper, 30 April 2022, 8 [34].
266 Statement of Renae Pepper, 30 April 2022, 8 [34]–9 [34].
270 Statement of Timothy Bullard, 10 May 2022, 30 [19d].
273 Consultation with non-government out of home care providers, 25 October 2021.
274 Consultation with non-government out of home care providers, 25 October 2021.
277 Child Safety Services, Assessing and Responding to Sexual Abuse Procedure (20 January 2022) 2.
278 Child Safety Services, Assessing and Responding to Sexual Abuse Procedure (20 January 2022) 2.
279 Child Safety Services, Assessing and Responding to Sexual Abuse Procedure (20 January 2022) 2.
281 Statement of Jonathan Higgins, 7 June 2022, 5 [10]–6 [14], 36 [169].
282 Statement of Renae Pepper, 30 April 2022, 9 [38]–10 [41].
283 Statement of Renae Pepper, 2 May 2022, 9 [38].
284 Statement of Jonathan Higgins, 7 June 2022, 21 [94].
287 Statement of Jenny Wing, 8 June 2022, 10 [45].
288 Consultation with Tasmania Police, 25 August 2021; Anonymous session, 17 November 2021.
291 Children, Young Persons and Their Families Act 1997 s 42(3)(a).
292 Statement of Dale Tolliday, 29 April 2022, 13 [58(b)].
293 Statement of Jenny Wing, 8 June 2022, 2 [11], 9 [35–37].
294 Children, Youth and Families Act 2005 (Vic) s 349(2).
295 Children, Youth and Families Act 2005 (Vic) s 349(3).
296 Children, Youth and Families Act 2005 (Vic) s 352.
297 Children, Youth and Families Act 2005 (Vic) s 354 (4).
298 Statement of Jenny Wing, 8 June 2022, 9 [40]–10 [41].
302 Statement of Jenny Wing, 8 June 2022, 2 [8], 3 [13].
303 Statement of Jenny Wing, 8 June 2022, 3 [13–14].
304 Statement of Jenny Wing, 8 June 2022, 3 [14], 6 [27], 7 [29].
305 Statement of Jenny Wing, 8 June 2022, 4 [19(e)], 6 [28(a)].
Acknowledgment of country
We acknowledge and pay respect to the Tasmanian Aboriginal people as the traditional and original owners, and continuing custodians of this land and acknowledge Elders, past and present.